Theis Skovsgaard Itenov, Anthony D Bai, Tor Biering-Sørensen, Amol Verma, Fahad Razak, Ajay Bhasin, Henning Bundgaard, Pradeesh Sivapalan, Kasper Iversen, Christian Rasmussen, Jens Rasmussen, Lotte Klitfod, Kathrine Dircks, Jens-Ulrik S Jensen, Mike Fralick
{"title":"克拉霉素与阿奇霉素对社区获得性肺炎和主要不良心血管事件风险的影响:一项来自加拿大和丹麦的多中心队列研究","authors":"Theis Skovsgaard Itenov, Anthony D Bai, Tor Biering-Sørensen, Amol Verma, Fahad Razak, Ajay Bhasin, Henning Bundgaard, Pradeesh Sivapalan, Kasper Iversen, Christian Rasmussen, Jens Rasmussen, Lotte Klitfod, Kathrine Dircks, Jens-Ulrik S Jensen, Mike Fralick","doi":"10.1002/pds.70163","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Studies suggest that clarithromycin is associated with an increased risk of major adverse cardiovascular events (MACE) among adults with coronary artery disease. However, data comparing clarithromycin to other macrolides, such as azithromycin, in a broader population are lacking.</p><p><strong>Methods: </strong>A multicenter study was conducted in 33 hospitals in Ontario, Canada, and Copenhagen, Denmark, using the Target Trial framework. Adults hospitalized with community-acquired pneumonia (CAP) who received either clarithromycin or azithromycin were included. The primary outcome was MACE, defined as the one-year risk of nonfatal myocardial infarction, nonfatal stroke, or all-cause mortality. Propensity score matching and Cox proportional hazards models were used for analysis.</p><p><strong>Results: </strong>In Ontario, we identified 23 081 patients with CAP, and 11 164 received oral macrolides. After propensity score matching, the primary outcome occurred in 7.8% of clarithromycin patients and 9.1% of azithromycin patients (HR 0.85, 95% CI 0.60-1.21). In Copenhagen, there were 11 280 patients with CAP and 3924 received oral macrolides. After propensity score matching, 19% of clarithromycin patients and 12% of azithromycin patients experienced the primary outcome for oral macrolides (HR 1.7, 95% CI 1.2-2.4, p = 0.002). Meta-analysis of the point estimate from each country provided an overall HR of 1.21 (95% CI 0.61-2.39). For intravenous macrolides in Copenhagen, the HR was 1.15 (95% CI 1.0-1.3, p = 0.007) for clarithromycin compared to azithromycin.</p><p><strong>Conclusion: </strong>This study did not consistently observe an increased risk of cardiovascular events with clarithromycin among adults hospitalized with CAP. However, the observational nature of the study may introduce selection bias and unmeasured confounding.</p>","PeriodicalId":19782,"journal":{"name":"Pharmacoepidemiology and Drug Safety","volume":"34 6","pages":"e70163"},"PeriodicalIF":2.4000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12144676/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clarithromycin Versus Azithromycin for Community-Acquired Pneumonia and the Risk of Major Adverse Cardiovascular Events: A Multicentre Cohort Study Using Data From Canada and Denmark.\",\"authors\":\"Theis Skovsgaard Itenov, Anthony D Bai, Tor Biering-Sørensen, Amol Verma, Fahad Razak, Ajay Bhasin, Henning Bundgaard, Pradeesh Sivapalan, Kasper Iversen, Christian Rasmussen, Jens Rasmussen, Lotte Klitfod, Kathrine Dircks, Jens-Ulrik S Jensen, Mike Fralick\",\"doi\":\"10.1002/pds.70163\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Studies suggest that clarithromycin is associated with an increased risk of major adverse cardiovascular events (MACE) among adults with coronary artery disease. However, data comparing clarithromycin to other macrolides, such as azithromycin, in a broader population are lacking.</p><p><strong>Methods: </strong>A multicenter study was conducted in 33 hospitals in Ontario, Canada, and Copenhagen, Denmark, using the Target Trial framework. Adults hospitalized with community-acquired pneumonia (CAP) who received either clarithromycin or azithromycin were included. The primary outcome was MACE, defined as the one-year risk of nonfatal myocardial infarction, nonfatal stroke, or all-cause mortality. Propensity score matching and Cox proportional hazards models were used for analysis.</p><p><strong>Results: </strong>In Ontario, we identified 23 081 patients with CAP, and 11 164 received oral macrolides. After propensity score matching, the primary outcome occurred in 7.8% of clarithromycin patients and 9.1% of azithromycin patients (HR 0.85, 95% CI 0.60-1.21). In Copenhagen, there were 11 280 patients with CAP and 3924 received oral macrolides. After propensity score matching, 19% of clarithromycin patients and 12% of azithromycin patients experienced the primary outcome for oral macrolides (HR 1.7, 95% CI 1.2-2.4, p = 0.002). Meta-analysis of the point estimate from each country provided an overall HR of 1.21 (95% CI 0.61-2.39). For intravenous macrolides in Copenhagen, the HR was 1.15 (95% CI 1.0-1.3, p = 0.007) for clarithromycin compared to azithromycin.</p><p><strong>Conclusion: </strong>This study did not consistently observe an increased risk of cardiovascular events with clarithromycin among adults hospitalized with CAP. However, the observational nature of the study may introduce selection bias and unmeasured confounding.</p>\",\"PeriodicalId\":19782,\"journal\":{\"name\":\"Pharmacoepidemiology and Drug Safety\",\"volume\":\"34 6\",\"pages\":\"e70163\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12144676/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pharmacoepidemiology and Drug Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/pds.70163\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacoepidemiology and Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pds.70163","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
摘要
背景:研究表明,克拉霉素与冠状动脉疾病成人主要不良心血管事件(MACE)的风险增加有关。然而,在更广泛的人群中比较克拉霉素和其他大环内酯类药物(如阿奇霉素)的数据缺乏。方法:采用目标试验框架,在加拿大安大略省和丹麦哥本哈根的33家医院进行了一项多中心研究。纳入了接受克拉霉素或阿奇霉素治疗的社区获得性肺炎(CAP)住院成人。主要终点是MACE,定义为非致死性心肌梗死、非致死性卒中或全因死亡率的一年风险。采用倾向评分匹配和Cox比例风险模型进行分析。结果:在安大略省,我们确定了23 081例CAP患者,其中11 164例接受口服大环内酯类药物治疗。倾向评分匹配后,主要结局发生在7.8%的克拉霉素患者和9.1%的阿奇霉素患者(HR 0.85, 95% CI 0.60-1.21)。在哥本哈根,有11280例CAP患者,3924例接受口服大环内酯类药物治疗。倾向评分匹配后,19%的克拉霉素患者和12%的阿奇霉素患者经历了口服大环内酯类药物的主要结局(HR 1.7, 95% CI 1.2-2.4, p = 0.002)。对每个国家的点估计值进行荟萃分析,总风险比为1.21 (95% CI 0.61-2.39)。哥本哈根静脉注射大环内酯类药物时,克拉霉素与阿奇霉素的风险比为1.15 (95% CI 1.0-1.3, p = 0.007)。结论:本研究并未一致观察到因CAP住院的成人患者使用克拉霉素会增加心血管事件的风险。然而,该研究的观察性可能会引入选择偏倚和未测量的混淆。
Clarithromycin Versus Azithromycin for Community-Acquired Pneumonia and the Risk of Major Adverse Cardiovascular Events: A Multicentre Cohort Study Using Data From Canada and Denmark.
Background: Studies suggest that clarithromycin is associated with an increased risk of major adverse cardiovascular events (MACE) among adults with coronary artery disease. However, data comparing clarithromycin to other macrolides, such as azithromycin, in a broader population are lacking.
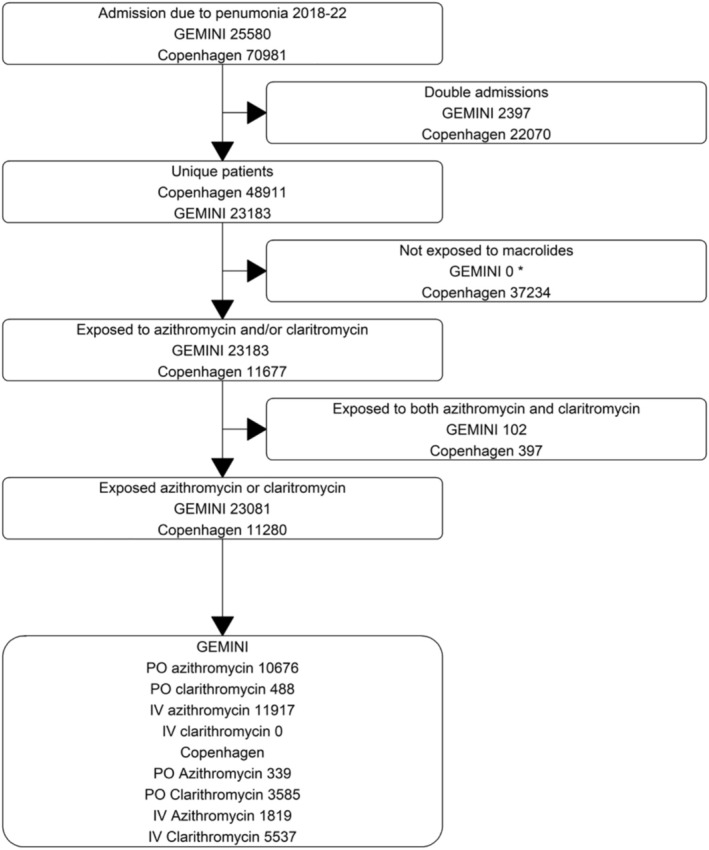
Methods: A multicenter study was conducted in 33 hospitals in Ontario, Canada, and Copenhagen, Denmark, using the Target Trial framework. Adults hospitalized with community-acquired pneumonia (CAP) who received either clarithromycin or azithromycin were included. The primary outcome was MACE, defined as the one-year risk of nonfatal myocardial infarction, nonfatal stroke, or all-cause mortality. Propensity score matching and Cox proportional hazards models were used for analysis.
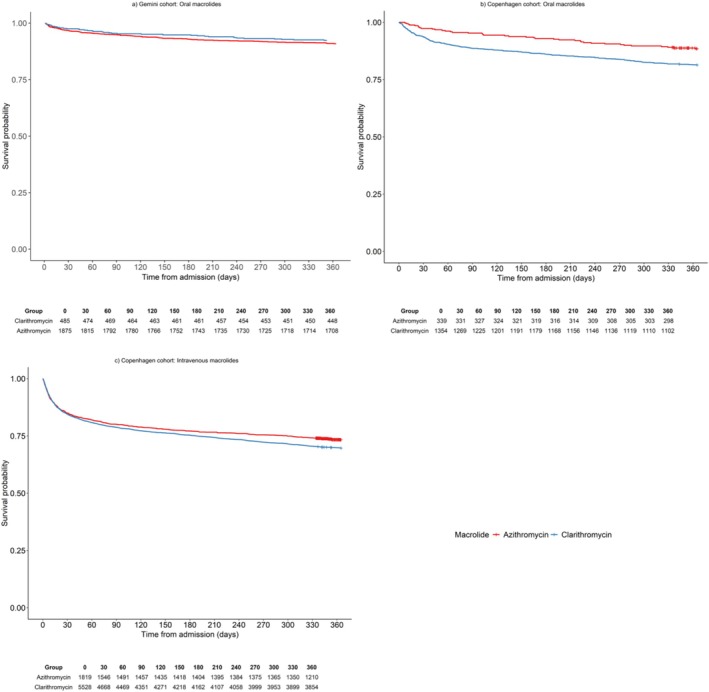
Results: In Ontario, we identified 23 081 patients with CAP, and 11 164 received oral macrolides. After propensity score matching, the primary outcome occurred in 7.8% of clarithromycin patients and 9.1% of azithromycin patients (HR 0.85, 95% CI 0.60-1.21). In Copenhagen, there were 11 280 patients with CAP and 3924 received oral macrolides. After propensity score matching, 19% of clarithromycin patients and 12% of azithromycin patients experienced the primary outcome for oral macrolides (HR 1.7, 95% CI 1.2-2.4, p = 0.002). Meta-analysis of the point estimate from each country provided an overall HR of 1.21 (95% CI 0.61-2.39). For intravenous macrolides in Copenhagen, the HR was 1.15 (95% CI 1.0-1.3, p = 0.007) for clarithromycin compared to azithromycin.
Conclusion: This study did not consistently observe an increased risk of cardiovascular events with clarithromycin among adults hospitalized with CAP. However, the observational nature of the study may introduce selection bias and unmeasured confounding.
期刊介绍:
The aim of Pharmacoepidemiology and Drug Safety is to provide an international forum for the communication and evaluation of data, methods and opinion in the discipline of pharmacoepidemiology. The Journal publishes peer-reviewed reports of original research, invited reviews and a variety of guest editorials and commentaries embracing scientific, medical, statistical, legal and economic aspects of pharmacoepidemiology and post-marketing surveillance of drug safety. Appropriate material in these categories may also be considered for publication as a Brief Report.
Particular areas of interest include:
design, analysis, results, and interpretation of studies looking at the benefit or safety of specific pharmaceuticals, biologics, or medical devices, including studies in pharmacovigilance, postmarketing surveillance, pharmacoeconomics, patient safety, molecular pharmacoepidemiology, or any other study within the broad field of pharmacoepidemiology;
comparative effectiveness research relating to pharmaceuticals, biologics, and medical devices. Comparative effectiveness research is the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, as these methods are truly used in the real world;
methodologic contributions of relevance to pharmacoepidemiology, whether original contributions, reviews of existing methods, or tutorials for how to apply the methods of pharmacoepidemiology;
assessments of harm versus benefit in drug therapy;
patterns of drug utilization;
relationships between pharmacoepidemiology and the formulation and interpretation of regulatory guidelines;
evaluations of risk management plans and programmes relating to pharmaceuticals, biologics and medical devices.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


