Elly Nuwamanya, Benjamin C Johnson, Stephen Okoboi, Ronald Galiwango, Diana Namuddu, Tabitha Ayabo, Joseph B Babigumira, Mohammed Lamorde
{"title":"预防艾滋病毒在乌干达垂直传播的强化保留战略:预算影响分析。","authors":"Elly Nuwamanya, Benjamin C Johnson, Stephen Okoboi, Ronald Galiwango, Diana Namuddu, Tabitha Ayabo, Joseph B Babigumira, Mohammed Lamorde","doi":"10.1007/s41669-025-00587-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Novel retention strategies have the potential to reduce vertical transmission of HIV and improve patient outcomes for women living with HIV (WLHIV) and their infants. We estimated the budget impact of the enhanced retention strategy (ERS) compared with the Ministry of Health strategy/standard of care (SOC) approach for preventing vertical transmission of HIV among women initiating antiretroviral therapy (ART) in late pregnancy in Uganda.</p><p><strong>Methods: </strong>A budget impact analysis (BIA) was conducted from the payer (Uganda's Ministry of Health) perspective with a 5-year time horizon. A Microsoft Excel-based BIA model was populated with HIV epidemiological data and expenditures from the literature and the clinical trial of dolutegravir in pregnant HIV mothers and their neonates. These cost projections accounted for various programmatic inputs, disease progression, differences in mortality based on treatment status, and subsequent pregnancies. The eligible population included all HIV-positive pregnant women currently receiving prevention of vertical transmission services in Uganda. The primary outcomes of the analysis were incremental budget costs, and infections averted over 5 years.</p><p><strong>Results: </strong>Adopting the ERS would lead to a net cost increase of US$63.8 million over the next 5 years, or a net cost increase of US$12.7 million per year compared with the SOC. Newly enrolled WLHIV accounts for US$39.5 million of these marginal costs, while in-system patients account for US$24.2 million. Direct programmatic costs of the ERS only account for 13% of this additional cost, with 87% of the marginal increase coming from the cost of providing ART for WLHIV who would otherwise be lost to follow-up. The ERS would avert an additional 6933 infant infections compared with the SOC.</p><p><strong>Conclusion: </strong>Implementing the ERS would significantly increase the Ugandan Ministry of Health's budget, but most additional costs would be accrued from the resulting expansion of ART client volume. The ERS is a relatively low-cost intervention to reduce loss to follow-up rates among marginalized and hard-to-reach populations.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"815-825"},"PeriodicalIF":2.1000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401848/pdf/","citationCount":"0","resultStr":"{\"title\":\"An Enhanced Retention Strategy to Prevent the Vertical Transmission of HIV in Uganda: A Budget Impact Analysis.\",\"authors\":\"Elly Nuwamanya, Benjamin C Johnson, Stephen Okoboi, Ronald Galiwango, Diana Namuddu, Tabitha Ayabo, Joseph B Babigumira, Mohammed Lamorde\",\"doi\":\"10.1007/s41669-025-00587-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Novel retention strategies have the potential to reduce vertical transmission of HIV and improve patient outcomes for women living with HIV (WLHIV) and their infants. We estimated the budget impact of the enhanced retention strategy (ERS) compared with the Ministry of Health strategy/standard of care (SOC) approach for preventing vertical transmission of HIV among women initiating antiretroviral therapy (ART) in late pregnancy in Uganda.</p><p><strong>Methods: </strong>A budget impact analysis (BIA) was conducted from the payer (Uganda's Ministry of Health) perspective with a 5-year time horizon. A Microsoft Excel-based BIA model was populated with HIV epidemiological data and expenditures from the literature and the clinical trial of dolutegravir in pregnant HIV mothers and their neonates. These cost projections accounted for various programmatic inputs, disease progression, differences in mortality based on treatment status, and subsequent pregnancies. The eligible population included all HIV-positive pregnant women currently receiving prevention of vertical transmission services in Uganda. The primary outcomes of the analysis were incremental budget costs, and infections averted over 5 years.</p><p><strong>Results: </strong>Adopting the ERS would lead to a net cost increase of US$63.8 million over the next 5 years, or a net cost increase of US$12.7 million per year compared with the SOC. Newly enrolled WLHIV accounts for US$39.5 million of these marginal costs, while in-system patients account for US$24.2 million. Direct programmatic costs of the ERS only account for 13% of this additional cost, with 87% of the marginal increase coming from the cost of providing ART for WLHIV who would otherwise be lost to follow-up. The ERS would avert an additional 6933 infant infections compared with the SOC.</p><p><strong>Conclusion: </strong>Implementing the ERS would significantly increase the Ugandan Ministry of Health's budget, but most additional costs would be accrued from the resulting expansion of ART client volume. The ERS is a relatively low-cost intervention to reduce loss to follow-up rates among marginalized and hard-to-reach populations.</p>\",\"PeriodicalId\":19770,\"journal\":{\"name\":\"PharmacoEconomics Open\",\"volume\":\" \",\"pages\":\"815-825\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401848/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PharmacoEconomics Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s41669-025-00587-x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-025-00587-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
An Enhanced Retention Strategy to Prevent the Vertical Transmission of HIV in Uganda: A Budget Impact Analysis.
Background: Novel retention strategies have the potential to reduce vertical transmission of HIV and improve patient outcomes for women living with HIV (WLHIV) and their infants. We estimated the budget impact of the enhanced retention strategy (ERS) compared with the Ministry of Health strategy/standard of care (SOC) approach for preventing vertical transmission of HIV among women initiating antiretroviral therapy (ART) in late pregnancy in Uganda.
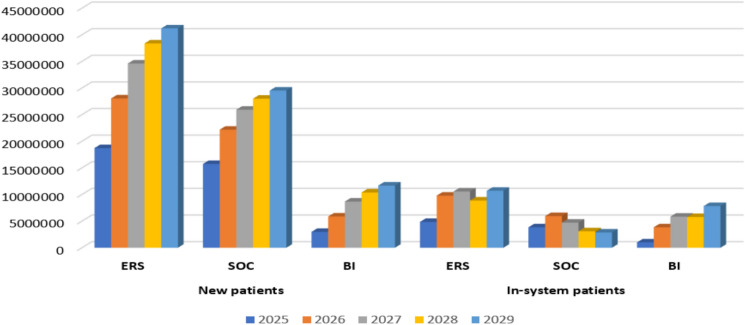
Methods: A budget impact analysis (BIA) was conducted from the payer (Uganda's Ministry of Health) perspective with a 5-year time horizon. A Microsoft Excel-based BIA model was populated with HIV epidemiological data and expenditures from the literature and the clinical trial of dolutegravir in pregnant HIV mothers and their neonates. These cost projections accounted for various programmatic inputs, disease progression, differences in mortality based on treatment status, and subsequent pregnancies. The eligible population included all HIV-positive pregnant women currently receiving prevention of vertical transmission services in Uganda. The primary outcomes of the analysis were incremental budget costs, and infections averted over 5 years.
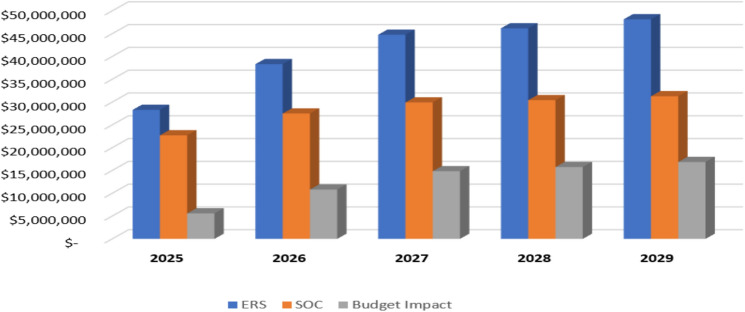
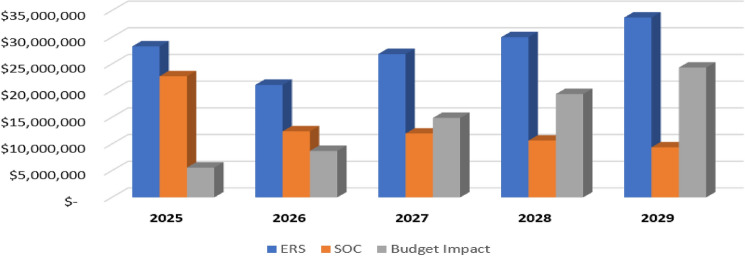
Results: Adopting the ERS would lead to a net cost increase of US$63.8 million over the next 5 years, or a net cost increase of US$12.7 million per year compared with the SOC. Newly enrolled WLHIV accounts for US$39.5 million of these marginal costs, while in-system patients account for US$24.2 million. Direct programmatic costs of the ERS only account for 13% of this additional cost, with 87% of the marginal increase coming from the cost of providing ART for WLHIV who would otherwise be lost to follow-up. The ERS would avert an additional 6933 infant infections compared with the SOC.
Conclusion: Implementing the ERS would significantly increase the Ugandan Ministry of Health's budget, but most additional costs would be accrued from the resulting expansion of ART client volume. The ERS is a relatively low-cost intervention to reduce loss to follow-up rates among marginalized and hard-to-reach populations.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


