Jesse P A Demandt, Thomas P Mast, Konrad A J van Beek, Arjan Koks, Marieke C V Bastiaansen, Pim A L Tonino, Marcel van 't Veer, Frederik M Zimmermann, Pieter-Jan Vlaar
{"title":"应用深度学习进行疑似急性冠状动脉综合征心电图解读的院前风险分层研究。","authors":"Jesse P A Demandt, Thomas P Mast, Konrad A J van Beek, Arjan Koks, Marieke C V Bastiaansen, Pim A L Tonino, Marcel van 't Veer, Frederik M Zimmermann, Pieter-Jan Vlaar","doi":"10.1136/bmjhci-2024-101292","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Most patients presenting with chest pain in the emergency medical services (EMS) setting are suspected of non-ST-elevation acute coronary syndrome (NSTE-ACS). Distinguishing true NSTE-ACS from non-cardiac chest pain based solely on the ECG is challenging. The aim of this study is to develop and validate a convolutional neural network (CNN)-based model for risk stratification of suspected NSTE-ACS patients and to compare its performance with currently available prehospital diagnostic tools.</p><p><strong>Methods: </strong>For this study, an internal training cohort and an external validation cohort were used, both consisting of suspected NSTE-ACS patients. A CNN (ECG interpretation by CNN (ECG-AI)) was trained and validated to detect NSTE-ACS. The diagnostic value of ECG-AI in detecting NSTE-ACS was compared with on-site ECG analyses by an EMS paramedic (ECG-EMS), point-of-care troponin assessment and a validated prehospital clinical risk score (prehospital History, ECG, Age, Risk factors and POC-troponin (preHEART)).</p><p><strong>Results: </strong>A total of 5645 patients suspected of NSTE-ACS were included. In the external validation cohort (n=754), 27% were diagnosed with NSTE-ACS. ECG-AI had a better diagnostic performance than ECG-EMS (area under the curve (AUROC) 0.70 (0.66 to 0.74) vs AUROC 0.65 (0.61 to 0.70), p=0.045) for diagnosing NSTE-ACS. The overall diagnostic accuracy of preHEART was AUROC 0.78 (0.74 to 0.82) and superior compared with ECG-AI (p=0.001). Incorporating ECG-AI into preHEART led to a significant improvement in diagnostic performance (AUROC 0.83 (0.79 to 0.86), p<0.001).</p><p><strong>Discussion: </strong>Correctly identifying patients who are at low risk for having NSTE-ACS is crucial for optimal triage in the prehospital setting. Recent studies have shown that these low-risk patients could potentially be left at home or transferred to a general practitioner, leading to less emergency department overcrowding and lower healthcare costs. Other studies demonstrated better overall diagnostic performance compared with our artificial intelligence (AI) model. However, these studies were aimed at a study population with a high prevalence of occlusive myocardial infarction, which could explain the differing levels of diagnostic performance.</p><p><strong>Conclusion: </strong>Integrating AI in prehospital ECG interpretation improves the identification of patients at low risk for having NSTE-ACS. Nonetheless, clinical risk scores currently yield the best diagnostic performance and their accuracy could be further enhanced through AI. Our results pave the way for new studies focused on exploring the role of AI in prehospital risk-stratification efforts.</p>","PeriodicalId":9050,"journal":{"name":"BMJ Health & Care Informatics","volume":"32 1","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-06-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12161418/pdf/","citationCount":"0","resultStr":"{\"title\":\"Towards prehospital risk stratification using deep learning for ECG interpretation in suspected acute coronary syndrome.\",\"authors\":\"Jesse P A Demandt, Thomas P Mast, Konrad A J van Beek, Arjan Koks, Marieke C V Bastiaansen, Pim A L Tonino, Marcel van 't Veer, Frederik M Zimmermann, Pieter-Jan Vlaar\",\"doi\":\"10.1136/bmjhci-2024-101292\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Most patients presenting with chest pain in the emergency medical services (EMS) setting are suspected of non-ST-elevation acute coronary syndrome (NSTE-ACS). Distinguishing true NSTE-ACS from non-cardiac chest pain based solely on the ECG is challenging. The aim of this study is to develop and validate a convolutional neural network (CNN)-based model for risk stratification of suspected NSTE-ACS patients and to compare its performance with currently available prehospital diagnostic tools.</p><p><strong>Methods: </strong>For this study, an internal training cohort and an external validation cohort were used, both consisting of suspected NSTE-ACS patients. A CNN (ECG interpretation by CNN (ECG-AI)) was trained and validated to detect NSTE-ACS. The diagnostic value of ECG-AI in detecting NSTE-ACS was compared with on-site ECG analyses by an EMS paramedic (ECG-EMS), point-of-care troponin assessment and a validated prehospital clinical risk score (prehospital History, ECG, Age, Risk factors and POC-troponin (preHEART)).</p><p><strong>Results: </strong>A total of 5645 patients suspected of NSTE-ACS were included. In the external validation cohort (n=754), 27% were diagnosed with NSTE-ACS. ECG-AI had a better diagnostic performance than ECG-EMS (area under the curve (AUROC) 0.70 (0.66 to 0.74) vs AUROC 0.65 (0.61 to 0.70), p=0.045) for diagnosing NSTE-ACS. The overall diagnostic accuracy of preHEART was AUROC 0.78 (0.74 to 0.82) and superior compared with ECG-AI (p=0.001). Incorporating ECG-AI into preHEART led to a significant improvement in diagnostic performance (AUROC 0.83 (0.79 to 0.86), p<0.001).</p><p><strong>Discussion: </strong>Correctly identifying patients who are at low risk for having NSTE-ACS is crucial for optimal triage in the prehospital setting. Recent studies have shown that these low-risk patients could potentially be left at home or transferred to a general practitioner, leading to less emergency department overcrowding and lower healthcare costs. Other studies demonstrated better overall diagnostic performance compared with our artificial intelligence (AI) model. However, these studies were aimed at a study population with a high prevalence of occlusive myocardial infarction, which could explain the differing levels of diagnostic performance.</p><p><strong>Conclusion: </strong>Integrating AI in prehospital ECG interpretation improves the identification of patients at low risk for having NSTE-ACS. Nonetheless, clinical risk scores currently yield the best diagnostic performance and their accuracy could be further enhanced through AI. Our results pave the way for new studies focused on exploring the role of AI in prehospital risk-stratification efforts.</p>\",\"PeriodicalId\":9050,\"journal\":{\"name\":\"BMJ Health & Care Informatics\",\"volume\":\"32 1\",\"pages\":\"\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-06-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12161418/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Health & Care Informatics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjhci-2024-101292\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Health & Care Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjhci-2024-101292","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Towards prehospital risk stratification using deep learning for ECG interpretation in suspected acute coronary syndrome.
Objectives: Most patients presenting with chest pain in the emergency medical services (EMS) setting are suspected of non-ST-elevation acute coronary syndrome (NSTE-ACS). Distinguishing true NSTE-ACS from non-cardiac chest pain based solely on the ECG is challenging. The aim of this study is to develop and validate a convolutional neural network (CNN)-based model for risk stratification of suspected NSTE-ACS patients and to compare its performance with currently available prehospital diagnostic tools.
Methods: For this study, an internal training cohort and an external validation cohort were used, both consisting of suspected NSTE-ACS patients. A CNN (ECG interpretation by CNN (ECG-AI)) was trained and validated to detect NSTE-ACS. The diagnostic value of ECG-AI in detecting NSTE-ACS was compared with on-site ECG analyses by an EMS paramedic (ECG-EMS), point-of-care troponin assessment and a validated prehospital clinical risk score (prehospital History, ECG, Age, Risk factors and POC-troponin (preHEART)).
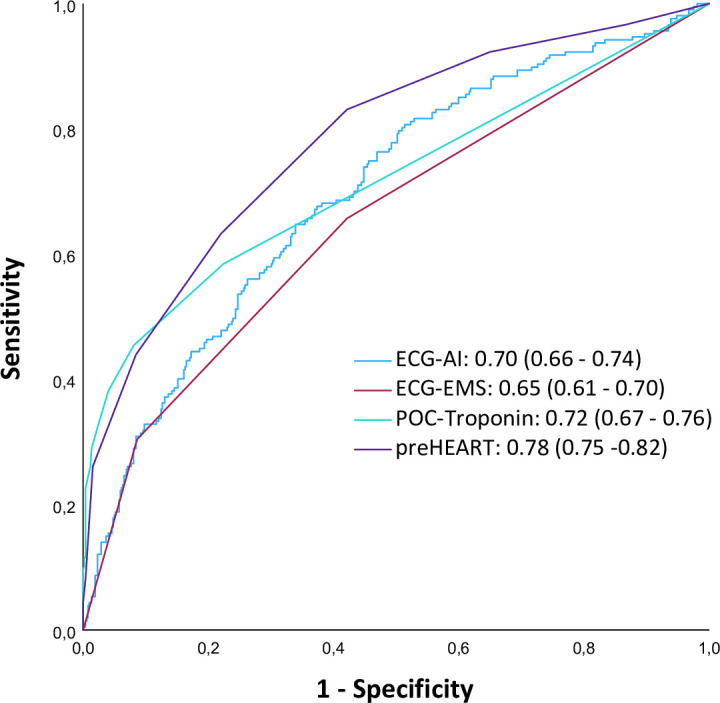
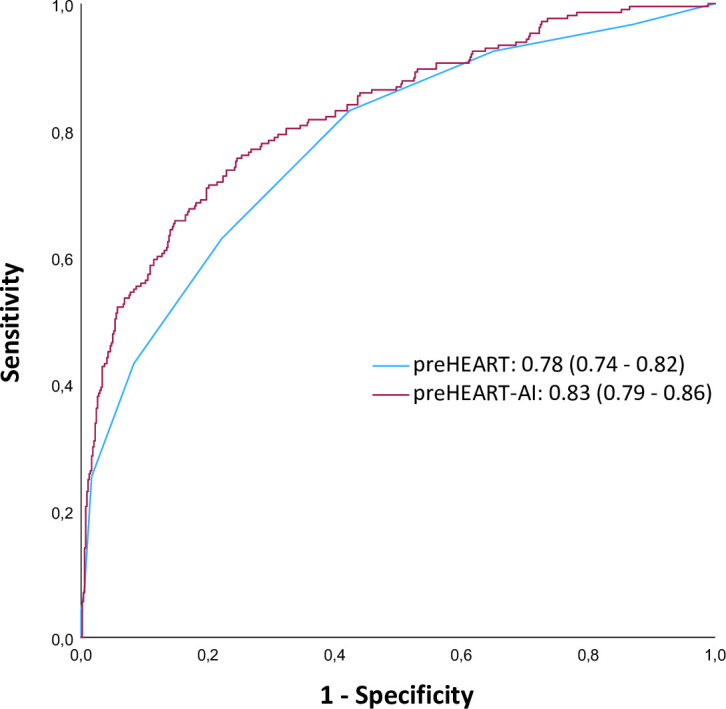
Results: A total of 5645 patients suspected of NSTE-ACS were included. In the external validation cohort (n=754), 27% were diagnosed with NSTE-ACS. ECG-AI had a better diagnostic performance than ECG-EMS (area under the curve (AUROC) 0.70 (0.66 to 0.74) vs AUROC 0.65 (0.61 to 0.70), p=0.045) for diagnosing NSTE-ACS. The overall diagnostic accuracy of preHEART was AUROC 0.78 (0.74 to 0.82) and superior compared with ECG-AI (p=0.001). Incorporating ECG-AI into preHEART led to a significant improvement in diagnostic performance (AUROC 0.83 (0.79 to 0.86), p<0.001).
Discussion: Correctly identifying patients who are at low risk for having NSTE-ACS is crucial for optimal triage in the prehospital setting. Recent studies have shown that these low-risk patients could potentially be left at home or transferred to a general practitioner, leading to less emergency department overcrowding and lower healthcare costs. Other studies demonstrated better overall diagnostic performance compared with our artificial intelligence (AI) model. However, these studies were aimed at a study population with a high prevalence of occlusive myocardial infarction, which could explain the differing levels of diagnostic performance.
Conclusion: Integrating AI in prehospital ECG interpretation improves the identification of patients at low risk for having NSTE-ACS. Nonetheless, clinical risk scores currently yield the best diagnostic performance and their accuracy could be further enhanced through AI. Our results pave the way for new studies focused on exploring the role of AI in prehospital risk-stratification efforts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


