Wallace T Miller, Scott Simpson, Shweta Sood, Michelle Hershman, Cheilonda R Johnson, James E Schmitt, Karen C Patterson
{"title":"肺间质纤维化影像学表型的频率。","authors":"Wallace T Miller, Scott Simpson, Shweta Sood, Michelle Hershman, Cheilonda R Johnson, James E Schmitt, Karen C Patterson","doi":"10.4102/sajr.v29i1.3098","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Evaluation of diffuse interstitial lung disease (ILD) in thoracic imaging is complicated. Radiologists often use a pattern approach to interpretation; however, they are rarely aware of the statistical frequency of disease presentation.</p><p><strong>Objectives: </strong>To evaluate the relative frequency of causes of fibrotic ILD as a function of imaging patterns.</p><p><strong>Method: </strong>A CT database of 396 cases of fibrotic ILD was amassed from an institutional diffuse lung disease registry and retrospective search of medical records. Three radiologists and one pulmonologist independently and blindly reviewed the CT scans for the distribution of fibrosis, predominant feature and non-pulmonary findings.</p><p><strong>Results: </strong>Peripheral fibrosis was most common (291/396, 73.5%), usually caused by idiopathic pulmonary fibrosis (IPF) and connective tissue diseases-related interstitial lung disease (CTD-ILD) but occasionally by hypersensitivity pneumonitis (HP), idiopathic nonspecific interstitial pneumonia (iNSIP) and asbestosis. Peripheral fibrosis with honeycombing was usually IPF and without honeycombing, was usually CTD-ILD. Peripheral fibrosis with pleural plaques was always asbestosis. Peripheral fibrosis with oesophageal dilatation was usually connective tissue diseases. Consolidative-like peripheral fibrosis was CTD-ILD. Axial fibrosis (61/396, 15.4%) was usually sarcoidosis, HP, CTD-ILD or silicosis. Axial fibrosis with predominantly consolidative-like fibrosis, honeycombing, or reticulation was usually sarcoidosis. Axial fibrosis predominated by ground glass opacity was usually HP or CTD-ILD. Lymph node calcification or short axis > 17 mm increased the probability that axial fibrosis was due to sarcoidosis. The non-specific fibrosis phenotype was uncommon (44/396, 11.1%), usually CTD-ILD (25/44, 57%) but also HP, IPF, iNSIP or asbestosis.</p><p><strong>Conclusion: </strong>Patterns of lung fibrosis provide guidelines to identify the cause.</p><p><strong>Contribution: </strong>A flow diagram that predicts the relative frequency of the causes of 10 patterns of ILD.</p>","PeriodicalId":43442,"journal":{"name":"SA Journal of Radiology","volume":"29 1","pages":"3098"},"PeriodicalIF":0.9000,"publicationDate":"2025-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12135718/pdf/","citationCount":"0","resultStr":"{\"title\":\"Frequency of imaging phenotypes of pulmonary interstitial fibrosis.\",\"authors\":\"Wallace T Miller, Scott Simpson, Shweta Sood, Michelle Hershman, Cheilonda R Johnson, James E Schmitt, Karen C Patterson\",\"doi\":\"10.4102/sajr.v29i1.3098\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Evaluation of diffuse interstitial lung disease (ILD) in thoracic imaging is complicated. Radiologists often use a pattern approach to interpretation; however, they are rarely aware of the statistical frequency of disease presentation.</p><p><strong>Objectives: </strong>To evaluate the relative frequency of causes of fibrotic ILD as a function of imaging patterns.</p><p><strong>Method: </strong>A CT database of 396 cases of fibrotic ILD was amassed from an institutional diffuse lung disease registry and retrospective search of medical records. Three radiologists and one pulmonologist independently and blindly reviewed the CT scans for the distribution of fibrosis, predominant feature and non-pulmonary findings.</p><p><strong>Results: </strong>Peripheral fibrosis was most common (291/396, 73.5%), usually caused by idiopathic pulmonary fibrosis (IPF) and connective tissue diseases-related interstitial lung disease (CTD-ILD) but occasionally by hypersensitivity pneumonitis (HP), idiopathic nonspecific interstitial pneumonia (iNSIP) and asbestosis. Peripheral fibrosis with honeycombing was usually IPF and without honeycombing, was usually CTD-ILD. Peripheral fibrosis with pleural plaques was always asbestosis. Peripheral fibrosis with oesophageal dilatation was usually connective tissue diseases. Consolidative-like peripheral fibrosis was CTD-ILD. Axial fibrosis (61/396, 15.4%) was usually sarcoidosis, HP, CTD-ILD or silicosis. Axial fibrosis with predominantly consolidative-like fibrosis, honeycombing, or reticulation was usually sarcoidosis. Axial fibrosis predominated by ground glass opacity was usually HP or CTD-ILD. Lymph node calcification or short axis > 17 mm increased the probability that axial fibrosis was due to sarcoidosis. The non-specific fibrosis phenotype was uncommon (44/396, 11.1%), usually CTD-ILD (25/44, 57%) but also HP, IPF, iNSIP or asbestosis.</p><p><strong>Conclusion: </strong>Patterns of lung fibrosis provide guidelines to identify the cause.</p><p><strong>Contribution: </strong>A flow diagram that predicts the relative frequency of the causes of 10 patterns of ILD.</p>\",\"PeriodicalId\":43442,\"journal\":{\"name\":\"SA Journal of Radiology\",\"volume\":\"29 1\",\"pages\":\"3098\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-05-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12135718/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SA Journal of Radiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4102/sajr.v29i1.3098\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SA Journal of Radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/sajr.v29i1.3098","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Frequency of imaging phenotypes of pulmonary interstitial fibrosis.
Background: Evaluation of diffuse interstitial lung disease (ILD) in thoracic imaging is complicated. Radiologists often use a pattern approach to interpretation; however, they are rarely aware of the statistical frequency of disease presentation.
Objectives: To evaluate the relative frequency of causes of fibrotic ILD as a function of imaging patterns.
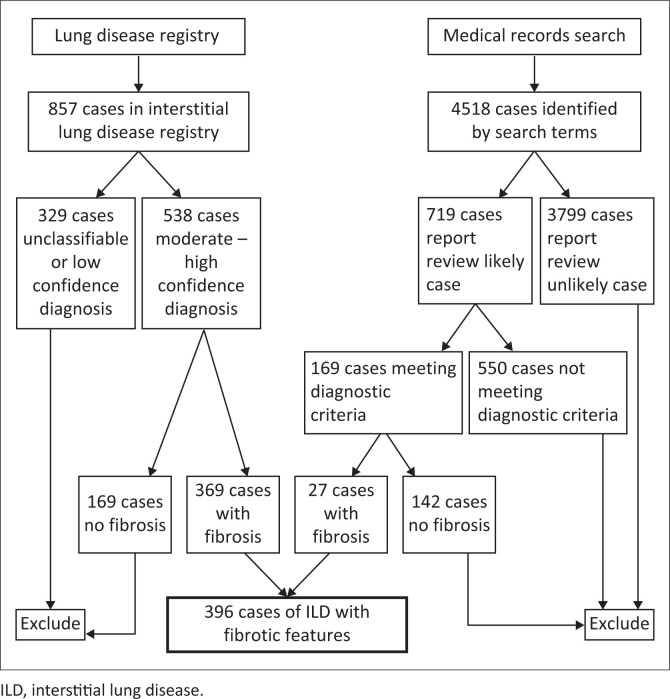
Method: A CT database of 396 cases of fibrotic ILD was amassed from an institutional diffuse lung disease registry and retrospective search of medical records. Three radiologists and one pulmonologist independently and blindly reviewed the CT scans for the distribution of fibrosis, predominant feature and non-pulmonary findings.
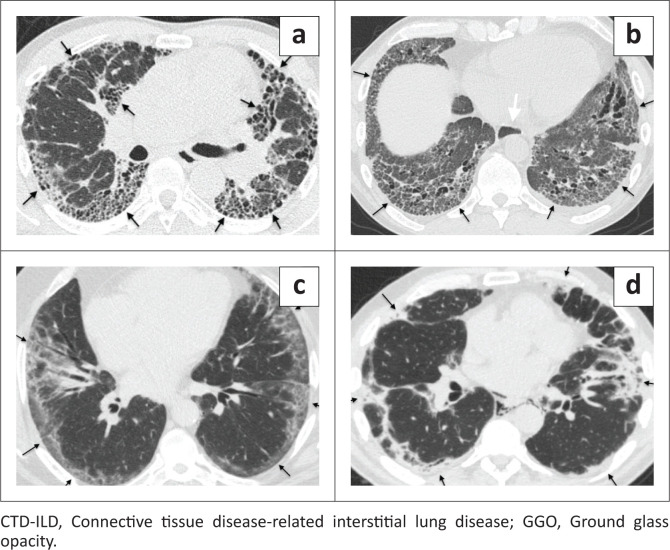
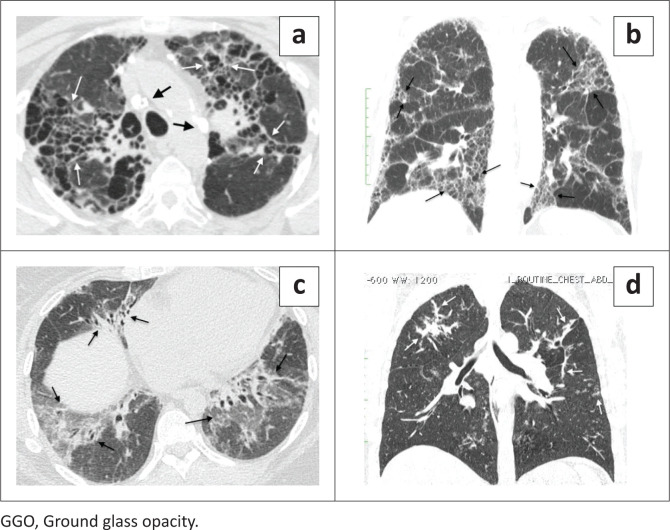
Results: Peripheral fibrosis was most common (291/396, 73.5%), usually caused by idiopathic pulmonary fibrosis (IPF) and connective tissue diseases-related interstitial lung disease (CTD-ILD) but occasionally by hypersensitivity pneumonitis (HP), idiopathic nonspecific interstitial pneumonia (iNSIP) and asbestosis. Peripheral fibrosis with honeycombing was usually IPF and without honeycombing, was usually CTD-ILD. Peripheral fibrosis with pleural plaques was always asbestosis. Peripheral fibrosis with oesophageal dilatation was usually connective tissue diseases. Consolidative-like peripheral fibrosis was CTD-ILD. Axial fibrosis (61/396, 15.4%) was usually sarcoidosis, HP, CTD-ILD or silicosis. Axial fibrosis with predominantly consolidative-like fibrosis, honeycombing, or reticulation was usually sarcoidosis. Axial fibrosis predominated by ground glass opacity was usually HP or CTD-ILD. Lymph node calcification or short axis > 17 mm increased the probability that axial fibrosis was due to sarcoidosis. The non-specific fibrosis phenotype was uncommon (44/396, 11.1%), usually CTD-ILD (25/44, 57%) but also HP, IPF, iNSIP or asbestosis.
Conclusion: Patterns of lung fibrosis provide guidelines to identify the cause.
Contribution: A flow diagram that predicts the relative frequency of the causes of 10 patterns of ILD.
期刊介绍:
The SA Journal of Radiology is the official journal of the Radiological Society of South Africa and the Professional Association of Radiologists in South Africa and Namibia. The SA Journal of Radiology is a general diagnostic radiological journal which carries original research and review articles, pictorial essays, case reports, letters, editorials, radiological practice and other radiological articles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



