Javaid Iqbal, Rahim Moineddin, Kieran L Quinn, Christopher M Booth, Craig C Earle, Stephanie Lheureux, Robert Grant, Jenny Lau, Lisa W Le, Peter Tanuseputro, James Downar, Gary Rodin, Hsien Seow, Jillian Tsai, Robert A Fowler, Breffni Hannon, Monika K Krzyzanowska, Camilla Zimmermann
{"title":"新型系统抗癌治疗和健康服务在成年癌症患者生命末期的使用。","authors":"Javaid Iqbal, Rahim Moineddin, Kieran L Quinn, Christopher M Booth, Craig C Earle, Stephanie Lheureux, Robert Grant, Jenny Lau, Lisa W Le, Peter Tanuseputro, James Downar, Gary Rodin, Hsien Seow, Jillian Tsai, Robert A Fowler, Breffni Hannon, Monika K Krzyzanowska, Camilla Zimmermann","doi":"10.1200/JCO-24-02816","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Use of chemotherapy at the end of life (EOL) is discouraged, but evidence to guide decisions on the use of novel systemic anticancer treatment (SACT) agents is lacking. We examined trends of use among SACT types and association with health services use at the EOL.</p><p><strong>Materials and methods: </strong>We analyzed Canadian Ontario Cancer Registry data for adults diagnosed with solid tumors or hematologic malignancies within 5 years of death who received SACT between March 2015 and March 2021. Receipt of SACT in the last 30 days of life was categorized as chemotherapy alone, chemotherapy and immunotherapy, immunotherapy alone, and targeted therapy alone. Outcomes included high health services use, including multiple (≥2) emergency department (ED) visits, multiple (≥2) hospitalizations, or any (≥1) intensive care unit admission, and hospital deaths. Segmented linear regression estimated monthly trends; multivariable logistic regression estimated adjusted odds ratios (aORs) of outcomes for various SACT types.</p><p><strong>Results: </strong>Among 68,963 patients, 18,337 (26.6%) received SACT at the EOL. From March 2015 to March 2020, use of SACT at the EOL increased (0.072% per month; <i>P</i> < .001), mainly driven by increased use of immunotherapy alone (0.064% per month; <i>P</i> < .001). Adjusted odds of high health services use and hospital death were more than two-fold greater among patients receiving SACT at the EOL (vs. none); individual aORs of high health services use and hospital death were 2.20 and 2.72 for chemotherapy alone, 2.36 and 3.10 for chemotherapy and immunotherapy, 1.92 and 2.27 for immunotherapy alone, and 1.75 and 2.37 for targeted therapy alone, respectively.</p><p><strong>Conclusion: </strong>Use of SACT at the EOL increased significantly over time, driven by increased use of immunotherapy. SACT use at the EOL, regardless of its type, was associated with high health services use and hospital death. Guidelines on the use of SACT at the EOL should include novel cancer treatments.</p>","PeriodicalId":15384,"journal":{"name":"Journal of Clinical Oncology","volume":" ","pages":"3279-3291"},"PeriodicalIF":41.9000,"publicationDate":"2025-10-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12527759/pdf/","citationCount":"0","resultStr":"{\"title\":\"Novel Systemic Anticancer Treatments and Health Services Use at the End of Life Among Adults With Cancer.\",\"authors\":\"Javaid Iqbal, Rahim Moineddin, Kieran L Quinn, Christopher M Booth, Craig C Earle, Stephanie Lheureux, Robert Grant, Jenny Lau, Lisa W Le, Peter Tanuseputro, James Downar, Gary Rodin, Hsien Seow, Jillian Tsai, Robert A Fowler, Breffni Hannon, Monika K Krzyzanowska, Camilla Zimmermann\",\"doi\":\"10.1200/JCO-24-02816\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Use of chemotherapy at the end of life (EOL) is discouraged, but evidence to guide decisions on the use of novel systemic anticancer treatment (SACT) agents is lacking. We examined trends of use among SACT types and association with health services use at the EOL.</p><p><strong>Materials and methods: </strong>We analyzed Canadian Ontario Cancer Registry data for adults diagnosed with solid tumors or hematologic malignancies within 5 years of death who received SACT between March 2015 and March 2021. Receipt of SACT in the last 30 days of life was categorized as chemotherapy alone, chemotherapy and immunotherapy, immunotherapy alone, and targeted therapy alone. Outcomes included high health services use, including multiple (≥2) emergency department (ED) visits, multiple (≥2) hospitalizations, or any (≥1) intensive care unit admission, and hospital deaths. Segmented linear regression estimated monthly trends; multivariable logistic regression estimated adjusted odds ratios (aORs) of outcomes for various SACT types.</p><p><strong>Results: </strong>Among 68,963 patients, 18,337 (26.6%) received SACT at the EOL. From March 2015 to March 2020, use of SACT at the EOL increased (0.072% per month; <i>P</i> < .001), mainly driven by increased use of immunotherapy alone (0.064% per month; <i>P</i> < .001). Adjusted odds of high health services use and hospital death were more than two-fold greater among patients receiving SACT at the EOL (vs. none); individual aORs of high health services use and hospital death were 2.20 and 2.72 for chemotherapy alone, 2.36 and 3.10 for chemotherapy and immunotherapy, 1.92 and 2.27 for immunotherapy alone, and 1.75 and 2.37 for targeted therapy alone, respectively.</p><p><strong>Conclusion: </strong>Use of SACT at the EOL increased significantly over time, driven by increased use of immunotherapy. SACT use at the EOL, regardless of its type, was associated with high health services use and hospital death. Guidelines on the use of SACT at the EOL should include novel cancer treatments.</p>\",\"PeriodicalId\":15384,\"journal\":{\"name\":\"Journal of Clinical Oncology\",\"volume\":\" \",\"pages\":\"3279-3291\"},\"PeriodicalIF\":41.9000,\"publicationDate\":\"2025-10-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12527759/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1200/JCO-24-02816\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1200/JCO-24-02816","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Novel Systemic Anticancer Treatments and Health Services Use at the End of Life Among Adults With Cancer.
Purpose: Use of chemotherapy at the end of life (EOL) is discouraged, but evidence to guide decisions on the use of novel systemic anticancer treatment (SACT) agents is lacking. We examined trends of use among SACT types and association with health services use at the EOL.
Materials and methods: We analyzed Canadian Ontario Cancer Registry data for adults diagnosed with solid tumors or hematologic malignancies within 5 years of death who received SACT between March 2015 and March 2021. Receipt of SACT in the last 30 days of life was categorized as chemotherapy alone, chemotherapy and immunotherapy, immunotherapy alone, and targeted therapy alone. Outcomes included high health services use, including multiple (≥2) emergency department (ED) visits, multiple (≥2) hospitalizations, or any (≥1) intensive care unit admission, and hospital deaths. Segmented linear regression estimated monthly trends; multivariable logistic regression estimated adjusted odds ratios (aORs) of outcomes for various SACT types.
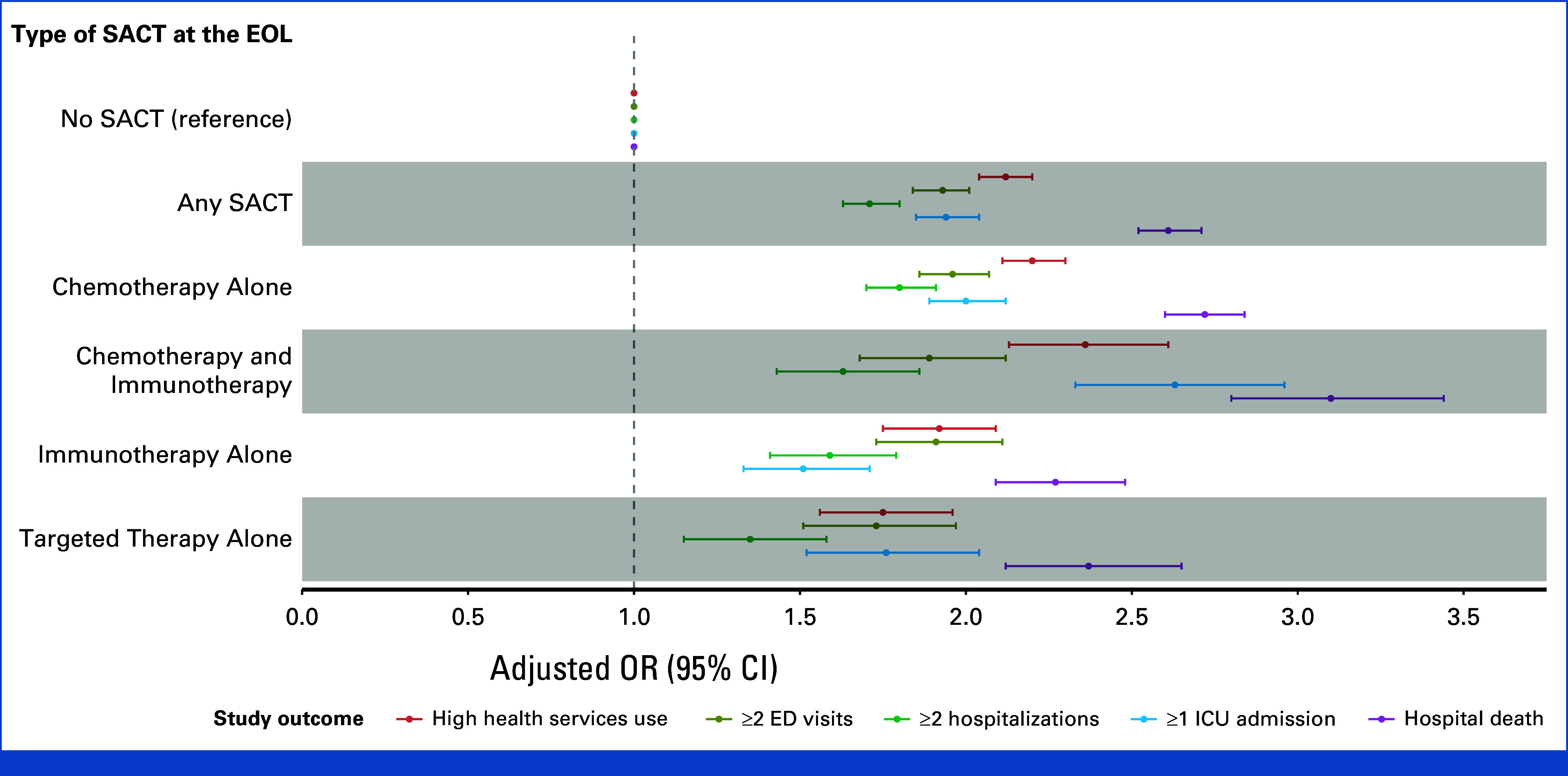
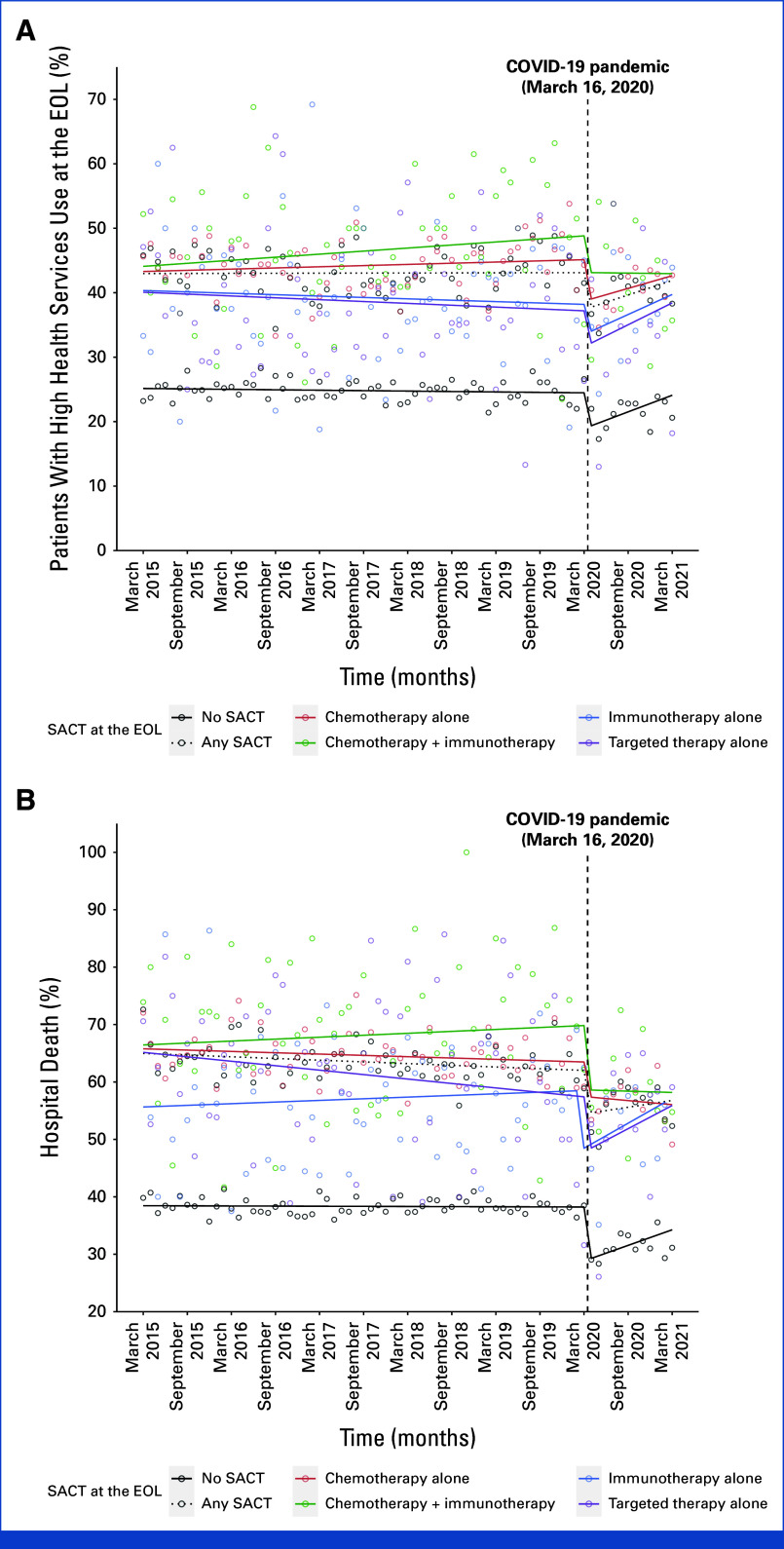
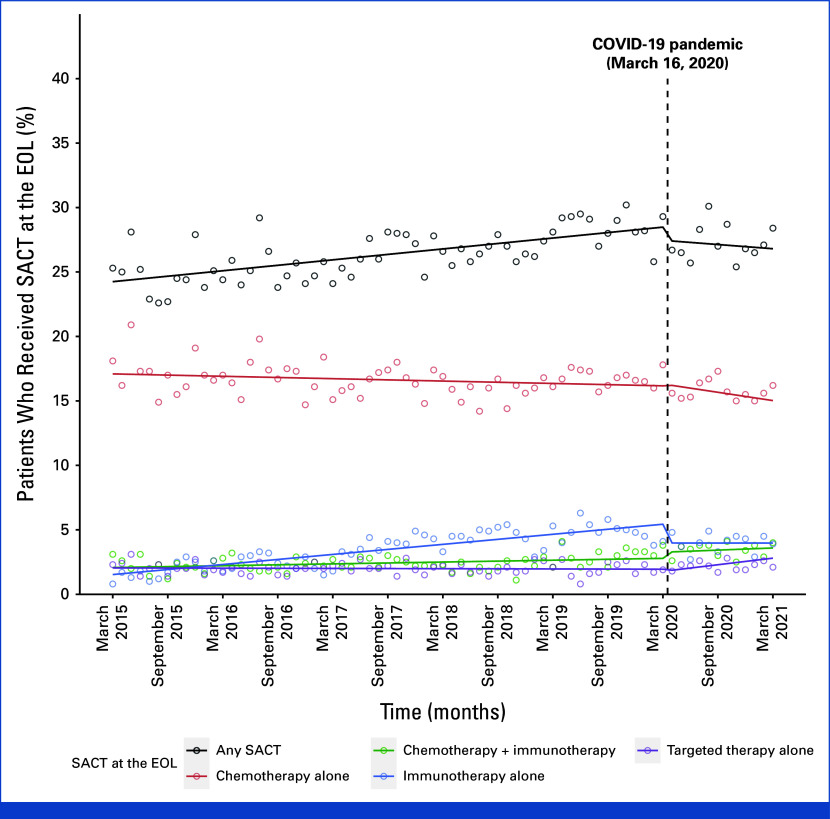
Results: Among 68,963 patients, 18,337 (26.6%) received SACT at the EOL. From March 2015 to March 2020, use of SACT at the EOL increased (0.072% per month; P < .001), mainly driven by increased use of immunotherapy alone (0.064% per month; P < .001). Adjusted odds of high health services use and hospital death were more than two-fold greater among patients receiving SACT at the EOL (vs. none); individual aORs of high health services use and hospital death were 2.20 and 2.72 for chemotherapy alone, 2.36 and 3.10 for chemotherapy and immunotherapy, 1.92 and 2.27 for immunotherapy alone, and 1.75 and 2.37 for targeted therapy alone, respectively.
Conclusion: Use of SACT at the EOL increased significantly over time, driven by increased use of immunotherapy. SACT use at the EOL, regardless of its type, was associated with high health services use and hospital death. Guidelines on the use of SACT at the EOL should include novel cancer treatments.
期刊介绍:
The Journal of Clinical Oncology serves its readers as the single most credible, authoritative resource for disseminating significant clinical oncology research. In print and in electronic format, JCO strives to publish the highest quality articles dedicated to clinical research. Original Reports remain the focus of JCO, but this scientific communication is enhanced by appropriately selected Editorials, Commentaries, Reviews, and other work that relate to the care of patients with cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


