Christina Sorbe, Secilay Kargin, Ralph von Kiedrowski, Diamant Thaci, Ansgar Weyergraf, Christine Blome, Matthias Augustin, Brigitte Stephan
{"title":"皮肤科医生对银屑病的全身药物选择是否与银屑病关节炎相容?数据来自德国国家牛皮癣登记处PsoBest。","authors":"Christina Sorbe, Secilay Kargin, Ralph von Kiedrowski, Diamant Thaci, Ansgar Weyergraf, Christine Blome, Matthias Augustin, Brigitte Stephan","doi":"10.2147/PTT.S524083","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Plaque-type psoriasis (PSO) is a chronic inflammatory systemic skin disease. Psoriatic arthritis (PsA) is a frequent component requiring early treatment to prevent joint damage. Guidelines recommend differentiated drug decisions for both conditions.</p><p><strong>Objective and methods: </strong>Descriptive analysis of drug choices for patients with PSO with or without additional PsA of the German Psoriasis registry PsoBest from 2007 to 2022.</p><p><strong>Results: </strong>The analysis comprises data of 17,310 patients with PSO: 18,6% with additional PsA (PSO+PsA), mean age 47.6 (± 14.8) years, 58.8% male, mean duration of PSO 16.4 years in patients without PsA (PSO-PsA; ± 14.3), 20.6 years in PSO+PsA (± 15.3, p < 0.001). PSO-PsA and PSO+PsA patients showed a marked burden of disease: PASI (15.7 (± 10.1) and 13.9 (± 10.6, p < 0.001)); DLQI (11.7 (± 7.2) and 12.3 (± 7.6; p < 0.001)). Before registry entry, 47.0% of patients received no systemic antipsoriatic treatment. Prior systemic medications were mainly non-biologics (40.4%), 12.6% were biologics, with a significantly higher rate in PSO+PsA patients (24.7% vs 9.8%). At registry baseline, the majority of the patients received non-biologic treatment (55.9%), with significantly higher rates for PSO-PsA patients (55.9% vs 34.8%). Biologics were used in 43.9% of all patients, with a significantly higher rate in PSO+PsA patients (65.9% vs 38.8%). Three hundred and three (9.4%) of PSO+PsA patients received treatments at baseline with approval for PSO, but not explicitly for PsA. Those patients had minor active joint involvement.</p><p><strong>Conclusion: </strong>Early and effective treatment of PsA is crucial to prevent persistent damage of the joints. Although most patients received recommended systemic treatment for PSO+PsA, there is a small number of patients with prescriptions addressing mainly the inflammation of the skin and not explicitly PsA. To choose recommended medication for both entities we need to regard the entire systemic inflammation and interdisciplinary co-working should be implemented.</p>","PeriodicalId":74589,"journal":{"name":"Psoriasis (Auckland, N.Z.)","volume":"15 ","pages":"197-207"},"PeriodicalIF":5.2000,"publicationDate":"2025-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12132669/pdf/","citationCount":"0","resultStr":"{\"title\":\"Are Systemic Drug Choices for Psoriasis by Dermatologists Compatible with Psoriatic Arthritis? Data from the German National Psoriasis Registry PsoBest.\",\"authors\":\"Christina Sorbe, Secilay Kargin, Ralph von Kiedrowski, Diamant Thaci, Ansgar Weyergraf, Christine Blome, Matthias Augustin, Brigitte Stephan\",\"doi\":\"10.2147/PTT.S524083\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Plaque-type psoriasis (PSO) is a chronic inflammatory systemic skin disease. Psoriatic arthritis (PsA) is a frequent component requiring early treatment to prevent joint damage. Guidelines recommend differentiated drug decisions for both conditions.</p><p><strong>Objective and methods: </strong>Descriptive analysis of drug choices for patients with PSO with or without additional PsA of the German Psoriasis registry PsoBest from 2007 to 2022.</p><p><strong>Results: </strong>The analysis comprises data of 17,310 patients with PSO: 18,6% with additional PsA (PSO+PsA), mean age 47.6 (± 14.8) years, 58.8% male, mean duration of PSO 16.4 years in patients without PsA (PSO-PsA; ± 14.3), 20.6 years in PSO+PsA (± 15.3, p < 0.001). PSO-PsA and PSO+PsA patients showed a marked burden of disease: PASI (15.7 (± 10.1) and 13.9 (± 10.6, p < 0.001)); DLQI (11.7 (± 7.2) and 12.3 (± 7.6; p < 0.001)). Before registry entry, 47.0% of patients received no systemic antipsoriatic treatment. Prior systemic medications were mainly non-biologics (40.4%), 12.6% were biologics, with a significantly higher rate in PSO+PsA patients (24.7% vs 9.8%). At registry baseline, the majority of the patients received non-biologic treatment (55.9%), with significantly higher rates for PSO-PsA patients (55.9% vs 34.8%). Biologics were used in 43.9% of all patients, with a significantly higher rate in PSO+PsA patients (65.9% vs 38.8%). Three hundred and three (9.4%) of PSO+PsA patients received treatments at baseline with approval for PSO, but not explicitly for PsA. Those patients had minor active joint involvement.</p><p><strong>Conclusion: </strong>Early and effective treatment of PsA is crucial to prevent persistent damage of the joints. Although most patients received recommended systemic treatment for PSO+PsA, there is a small number of patients with prescriptions addressing mainly the inflammation of the skin and not explicitly PsA. To choose recommended medication for both entities we need to regard the entire systemic inflammation and interdisciplinary co-working should be implemented.</p>\",\"PeriodicalId\":74589,\"journal\":{\"name\":\"Psoriasis (Auckland, N.Z.)\",\"volume\":\"15 \",\"pages\":\"197-207\"},\"PeriodicalIF\":5.2000,\"publicationDate\":\"2025-05-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12132669/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Psoriasis (Auckland, N.Z.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/PTT.S524083\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Psoriasis (Auckland, N.Z.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/PTT.S524083","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:斑块型银屑病(PSO)是一种慢性炎症性全身性皮肤病。银屑病关节炎(PsA)是一种常见的成分,需要早期治疗,以防止关节损伤。指南建议针对这两种情况做出不同的药物决定。目的和方法:描述性分析2007年至2022年德国银屑病登记处PsoBest中伴有或不伴有额外PsA的PSO患者的药物选择。结果:本研究纳入了17310例PSO患者的数据:18.6%伴有额外PsA (PSO+PsA),平均年龄47.6(±14.8)岁,58.8%为男性,无PsA (PSO-PsA)患者平均PSO病程16.4年;±14.3年),PSO+PsA组为20.6年(±15.3年,p < 0.001)。PSO-PsA和PSO+PsA患者的疾病负担显著:PASI(15.7(±10.1)和13.9(±10.6,p < 0.001));DLQI分别为11.7(±7.2)和12.3(±7.6);P < 0.001))。在登记前,47.0%的患者未接受全身抗银屑病治疗。既往全身性用药主要为非生物制剂(40.4%),12.6%为生物制剂,PSO+PsA患者的比例明显更高(24.7% vs 9.8%)。在注册基线,大多数患者接受了非生物治疗(55.9%),PSO-PsA患者的比例明显更高(55.9%对34.8%)。43.9%的患者使用了生物制剂,PSO+PsA患者的比例明显更高(65.9% vs 38.8%)。303名(9.4%)PSO+PsA患者在基线时接受了PSO批准的治疗,但没有明确针对PsA。这些患者有轻微的主动关节受累。结论:早期有效治疗是预防关节持续性损伤的关键。尽管大多数患者接受了PSO+PsA推荐的全身治疗,但也有少数患者的处方主要针对皮肤炎症,而不是明确针对PsA。在选择两种实体的推荐药物时,我们需要考虑整个系统性炎症,并应实施跨学科合作。
Are Systemic Drug Choices for Psoriasis by Dermatologists Compatible with Psoriatic Arthritis? Data from the German National Psoriasis Registry PsoBest.
Background: Plaque-type psoriasis (PSO) is a chronic inflammatory systemic skin disease. Psoriatic arthritis (PsA) is a frequent component requiring early treatment to prevent joint damage. Guidelines recommend differentiated drug decisions for both conditions.
Objective and methods: Descriptive analysis of drug choices for patients with PSO with or without additional PsA of the German Psoriasis registry PsoBest from 2007 to 2022.
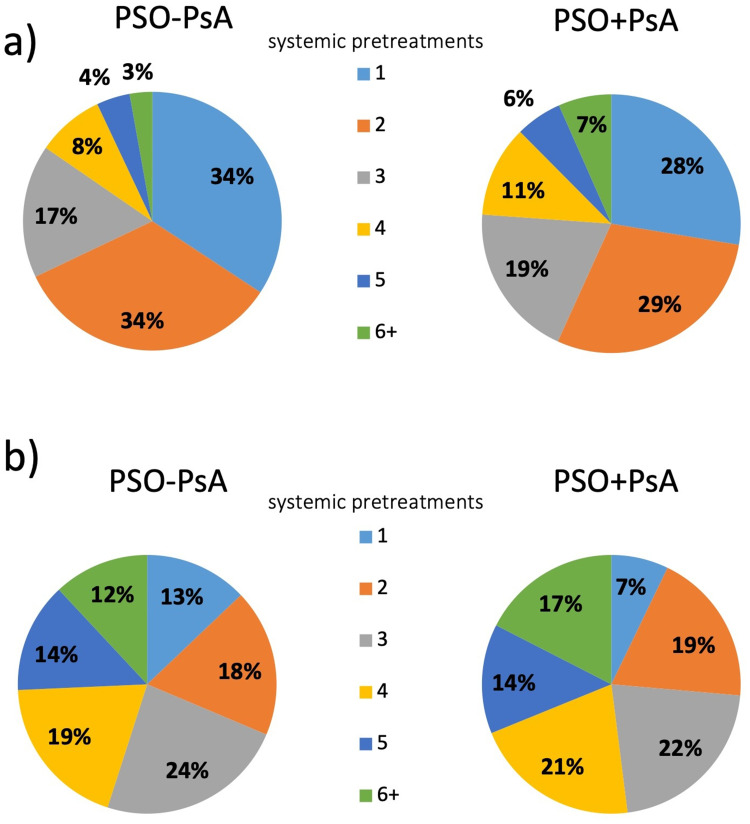
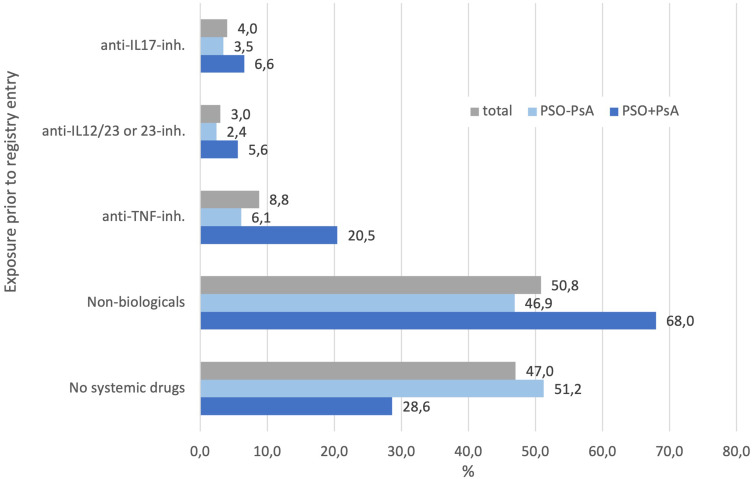
Results: The analysis comprises data of 17,310 patients with PSO: 18,6% with additional PsA (PSO+PsA), mean age 47.6 (± 14.8) years, 58.8% male, mean duration of PSO 16.4 years in patients without PsA (PSO-PsA; ± 14.3), 20.6 years in PSO+PsA (± 15.3, p < 0.001). PSO-PsA and PSO+PsA patients showed a marked burden of disease: PASI (15.7 (± 10.1) and 13.9 (± 10.6, p < 0.001)); DLQI (11.7 (± 7.2) and 12.3 (± 7.6; p < 0.001)). Before registry entry, 47.0% of patients received no systemic antipsoriatic treatment. Prior systemic medications were mainly non-biologics (40.4%), 12.6% were biologics, with a significantly higher rate in PSO+PsA patients (24.7% vs 9.8%). At registry baseline, the majority of the patients received non-biologic treatment (55.9%), with significantly higher rates for PSO-PsA patients (55.9% vs 34.8%). Biologics were used in 43.9% of all patients, with a significantly higher rate in PSO+PsA patients (65.9% vs 38.8%). Three hundred and three (9.4%) of PSO+PsA patients received treatments at baseline with approval for PSO, but not explicitly for PsA. Those patients had minor active joint involvement.
Conclusion: Early and effective treatment of PsA is crucial to prevent persistent damage of the joints. Although most patients received recommended systemic treatment for PSO+PsA, there is a small number of patients with prescriptions addressing mainly the inflammation of the skin and not explicitly PsA. To choose recommended medication for both entities we need to regard the entire systemic inflammation and interdisciplinary co-working should be implemented.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


