{"title":"贫血和慢性肾脏疾病对经皮冠状动脉介入治疗后结果的双重影响:来自日本全国登记的见解","authors":"Ryoma Fukuoka, Kyohei Yamaji, Shun Kohsaka, Hideki Ishii, Yuichiro Mori, Yohei Numasawa, Tetsu Watanabe, Takashi Nakayama, Koichiro Sugimura, Yoshihide Fujimoto, Masaki Ieda, Akio Kawamura, Tetsuya Amano, Ken Kozuma","doi":"10.1136/openhrt-2024-003146","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anaemia and chronic kidney disease (CKD) are both established risk factors for bleeding events after percutaneous coronary intervention (PCI). These conditions often coexist; however, previous assessments of these factors individually may have led to an underestimation of their impact on clinical outcomes.</p><p><strong>Methods: </strong>We analysed the data of 77 482 patients who underwent PCI between 2017 and 2020 in the Japanese nationwide PCI registry. Based on preprocedural anaemia (haemoglobin: <13 g/dL in men; <12 g/dL in women) and CKD (estimated glomerular filtration rate, <60 mL/min/1.73 m²) statuses, the patients were categorised into 'neither anaemia nor CKD' (n=36 629; 47.3%), 'CKD alone' (n=17 120; 22.1%), 'anaemia alone' (n=10 136; 13.1%) and 'both anaemia and CKD' (n=13 597; 17.5%) groups. The study endpoints included bleeding (fatal or non-fatal major bleeding) and ischaemic (cardiovascular death, non-fatal acute coronary syndrome or non-fatal ischaemic stroke) events.</p><p><strong>Results: </strong>The 1-year incidence of bleeding and ischaemic events was highest in the 'both anaemia and CKD' group and lowest in the 'neither anaemia nor CKD' group. After adjustment, 'anaemia alone' (HR 1.52; 95% CI 1.29 to 1.79; p<0.001) and 'both anaemia and CKD' (HR 1.39; 95% CI 1.18 to 1.63; p<0.001), but not 'CKD alone' (HR 1.00; 95% CI 0.85 to 1.17; p=0.97), were significantly associated with high risks of bleeding events compared with 'neither anaemia nor CKD'. All three groups had higher ischaemic risk compared with 'neither anaemia nor CKD' ('CKD alone': HR 1.29; 95% CI 1.16 to 1.45; p<0.001, 'anaemia alone': HR 1.40; 95% CI 1.22 to 1.60; p<0.001, 'both anaemia and CKD': HR 1.61; 95% CI 1.43 to 1.81; p<0.001).</p><p><strong>Conclusions: </strong>Anaemia increased bleeding risk regardless of CKD status, whereas 'CKD alone' did not. In addition, patients with anaemia and/or CKD were at a higher risk of ischaemic events. Clinicians should routinely perform initial risk assessments stratified by anaemia and CKD for patients undergoing PCI.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 1","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12142070/pdf/","citationCount":"0","resultStr":"{\"title\":\"Dual impact of anaemia and chronic kidney disease on postpercutaneous coronary intervention outcomes: insights from the Japanese nationwide registry.\",\"authors\":\"Ryoma Fukuoka, Kyohei Yamaji, Shun Kohsaka, Hideki Ishii, Yuichiro Mori, Yohei Numasawa, Tetsu Watanabe, Takashi Nakayama, Koichiro Sugimura, Yoshihide Fujimoto, Masaki Ieda, Akio Kawamura, Tetsuya Amano, Ken Kozuma\",\"doi\":\"10.1136/openhrt-2024-003146\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Anaemia and chronic kidney disease (CKD) are both established risk factors for bleeding events after percutaneous coronary intervention (PCI). These conditions often coexist; however, previous assessments of these factors individually may have led to an underestimation of their impact on clinical outcomes.</p><p><strong>Methods: </strong>We analysed the data of 77 482 patients who underwent PCI between 2017 and 2020 in the Japanese nationwide PCI registry. Based on preprocedural anaemia (haemoglobin: <13 g/dL in men; <12 g/dL in women) and CKD (estimated glomerular filtration rate, <60 mL/min/1.73 m²) statuses, the patients were categorised into 'neither anaemia nor CKD' (n=36 629; 47.3%), 'CKD alone' (n=17 120; 22.1%), 'anaemia alone' (n=10 136; 13.1%) and 'both anaemia and CKD' (n=13 597; 17.5%) groups. The study endpoints included bleeding (fatal or non-fatal major bleeding) and ischaemic (cardiovascular death, non-fatal acute coronary syndrome or non-fatal ischaemic stroke) events.</p><p><strong>Results: </strong>The 1-year incidence of bleeding and ischaemic events was highest in the 'both anaemia and CKD' group and lowest in the 'neither anaemia nor CKD' group. After adjustment, 'anaemia alone' (HR 1.52; 95% CI 1.29 to 1.79; p<0.001) and 'both anaemia and CKD' (HR 1.39; 95% CI 1.18 to 1.63; p<0.001), but not 'CKD alone' (HR 1.00; 95% CI 0.85 to 1.17; p=0.97), were significantly associated with high risks of bleeding events compared with 'neither anaemia nor CKD'. All three groups had higher ischaemic risk compared with 'neither anaemia nor CKD' ('CKD alone': HR 1.29; 95% CI 1.16 to 1.45; p<0.001, 'anaemia alone': HR 1.40; 95% CI 1.22 to 1.60; p<0.001, 'both anaemia and CKD': HR 1.61; 95% CI 1.43 to 1.81; p<0.001).</p><p><strong>Conclusions: </strong>Anaemia increased bleeding risk regardless of CKD status, whereas 'CKD alone' did not. In addition, patients with anaemia and/or CKD were at a higher risk of ischaemic events. Clinicians should routinely perform initial risk assessments stratified by anaemia and CKD for patients undergoing PCI.</p>\",\"PeriodicalId\":19505,\"journal\":{\"name\":\"Open Heart\",\"volume\":\"12 1\",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-06-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12142070/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Heart\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/openhrt-2024-003146\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2024-003146","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:贫血和慢性肾脏疾病(CKD)都是经皮冠状动脉介入治疗(PCI)后出血事件的危险因素。这些条件经常共存;然而,先前对这些因素的单独评估可能导致低估了它们对临床结果的影响。方法:我们分析了2017年至2020年在日本全国PCI登记处接受PCI治疗的77482例患者的数据。基于手术前贫血(血红蛋白):结果:1年出血和缺血事件的发生率在“贫血和CKD”组最高,在“无贫血和CKD”组最低。调整后,“仅贫血”(HR 1.52;95% CI 1.29 - 1.79;结论:无论CKD状态如何,贫血都会增加出血风险,而单纯CKD则不会。此外,患有贫血和/或CKD的患者发生缺血性事件的风险更高。临床医生应该对接受PCI的患者按贫血和CKD分层进行常规的初始风险评估。
Dual impact of anaemia and chronic kidney disease on postpercutaneous coronary intervention outcomes: insights from the Japanese nationwide registry.
Background: Anaemia and chronic kidney disease (CKD) are both established risk factors for bleeding events after percutaneous coronary intervention (PCI). These conditions often coexist; however, previous assessments of these factors individually may have led to an underestimation of their impact on clinical outcomes.
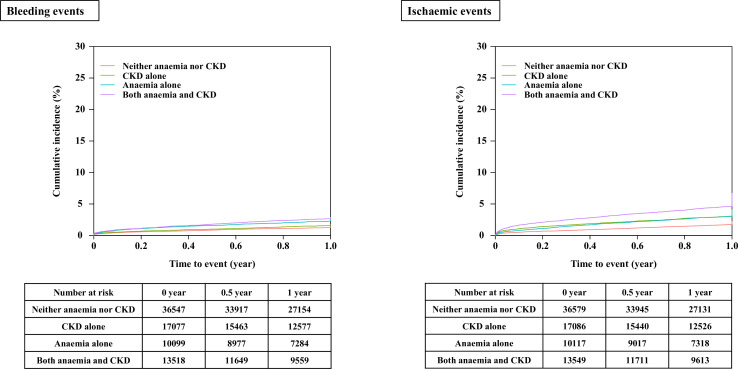
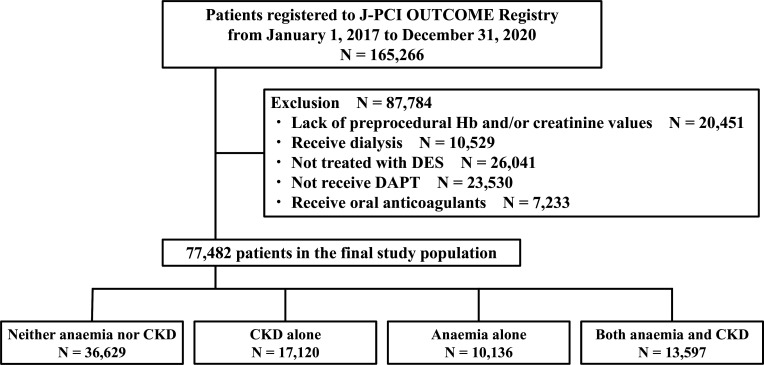
Methods: We analysed the data of 77 482 patients who underwent PCI between 2017 and 2020 in the Japanese nationwide PCI registry. Based on preprocedural anaemia (haemoglobin: <13 g/dL in men; <12 g/dL in women) and CKD (estimated glomerular filtration rate, <60 mL/min/1.73 m²) statuses, the patients were categorised into 'neither anaemia nor CKD' (n=36 629; 47.3%), 'CKD alone' (n=17 120; 22.1%), 'anaemia alone' (n=10 136; 13.1%) and 'both anaemia and CKD' (n=13 597; 17.5%) groups. The study endpoints included bleeding (fatal or non-fatal major bleeding) and ischaemic (cardiovascular death, non-fatal acute coronary syndrome or non-fatal ischaemic stroke) events.
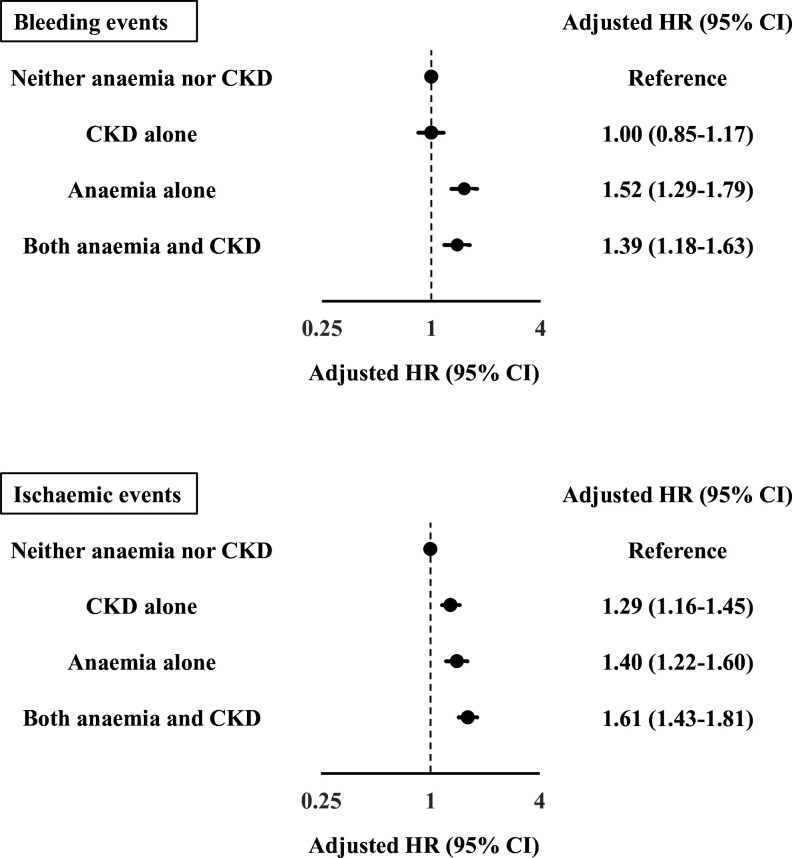
Results: The 1-year incidence of bleeding and ischaemic events was highest in the 'both anaemia and CKD' group and lowest in the 'neither anaemia nor CKD' group. After adjustment, 'anaemia alone' (HR 1.52; 95% CI 1.29 to 1.79; p<0.001) and 'both anaemia and CKD' (HR 1.39; 95% CI 1.18 to 1.63; p<0.001), but not 'CKD alone' (HR 1.00; 95% CI 0.85 to 1.17; p=0.97), were significantly associated with high risks of bleeding events compared with 'neither anaemia nor CKD'. All three groups had higher ischaemic risk compared with 'neither anaemia nor CKD' ('CKD alone': HR 1.29; 95% CI 1.16 to 1.45; p<0.001, 'anaemia alone': HR 1.40; 95% CI 1.22 to 1.60; p<0.001, 'both anaemia and CKD': HR 1.61; 95% CI 1.43 to 1.81; p<0.001).
Conclusions: Anaemia increased bleeding risk regardless of CKD status, whereas 'CKD alone' did not. In addition, patients with anaemia and/or CKD were at a higher risk of ischaemic events. Clinicians should routinely perform initial risk assessments stratified by anaemia and CKD for patients undergoing PCI.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


