Naomi Holman, Claire M. Buckley, Lisa Devine, Kate Gajewska, Sean F. Dinneen, the Chronic Disease Data System Consortium
{"title":"爱尔兰需要一个全面的糖尿病数据系统。","authors":"Naomi Holman, Claire M. Buckley, Lisa Devine, Kate Gajewska, Sean F. Dinneen, the Chronic Disease Data System Consortium","doi":"10.1111/jdi.70080","DOIUrl":null,"url":null,"abstract":"<p>The primary purpose of healthcare systems is to prevent and treat disease. The mainstay of this is direct patient clinical care, but the system needs to be supported by reliable and timely data to function in an evidence-based and responsive way<span><sup>1</sup></span>. Many health systems around the globe have a rich tradition of using data to inform and improve care processes<span><sup>2-4</sup></span>. In Ireland, there is currently no single source of data that can reliably report the number of people living with diabetes and no collation of records that provides an overview of the care received and outcomes experienced by people living with diabetes. A dual payer (public/private) system has led to diverse models of care, with a substantial proportion of diabetes care being provided privately by general practitioners. Historically, the lack of a unique identifier makes linkage of (clinical and administrative) data systems challenging. Many questions remain unanswered, and the scope to improve services and health-services planning is hindered without mechanisms to monitor change. Issues of equity and equality remain hidden, and the perspectives of people within the health service on the characteristics and outcomes of people living with diabetes cannot be substantiated by data.</p><p>Without a comprehensive data system, there is no scope to verify (or disprove) perceptions and changes to services that may be made with limited data to support their evaluation; plans are not evidence-based, and data to prioritize and shape policymaking are lacking.</p><p>Currently, aspects of diabetes care are captured in several national administrative datasets, including records of prescriptions dispensed by community pharmacies, publicly funded hospital admissions, Chronic Disease Management (CDM) programme returns by General Practitioners, Diabetic RetinaScreen, and civil death registrations. The combination of public and private care provision in the Irish health service (Figure 1) means that coverage of the datasets is not always universal. Data analysis is limited by a lack of governance, infrastructure, and public engagement that facilitates continuous networked dataset linkage. A national individual health identifier (IHI) has been created, but full implementation requires further legislation. Additionally, some crucial data on the care and outcomes of people with diabetes, such as laboratory tests, anthropometric measures, and lifestyle risk factors, are held in local or sub-national systems, which vary in their compatibility. The need for a diabetes data system has been consistently identified and has the support of the Department of Health, the Health Service Executive (HSE), Diabetes Ireland (national patient organization) and academic organizations. With early funding allocated and posts being filled in 2025, processes are being established to provide clinical leadership, programme management, data management, analysis, and reporting functions.</p><p>To address the gap in data on diabetes care in Ireland, the HSE initiated a programme of work to create a diabetes data system. It will collate administrative data currently used within the health system to identify people with diagnosed diabetes and document their healthcare delivery and outcomes. It aims to be an exemplar that can be applied to other chronic diseases (Figure 2).</p><p>By utilizing existing datasets, the diabetes data system will minimize the burden for clinical staff. It will include the scope to assess the incidence and prevalence of diabetes, the level and variation in care received by people with diabetes, leading to an understanding of equity and equality in healthcare. It will become dynamic by supporting service activity metrics, quality assessment/awareness, improvement of services to enable planning, monitoring, and evaluation, and the generation of new knowledge through scientific methodologies. As the role of real-world data in academic research grows, the data system will provide a rich dataset to explore the epidemiology and health economics of diabetes. In the long term, there is an aspiration of becoming a learning health system moving toward a real-time clinical and administrative data system accessible at the point of clinical care.</p><p>The journey from concept to a fully functioning data system will take many steps. A governance structure is needed to implement and oversee the work programme. The formal structure should include a senior leadership group that sets, guides, and monitors the strategic direction of the health service. An implementation group is required that will focus on the delivery of the data system; appropriate analysis and engagement with the diabetes community is also needed. At all levels, the governance system should be able to make decisions, solve problems, maintain support for the development of the data system, and ensure it meets its specified functions. As described in Figure 2, the function of the data system will vary across user groups. The clinical community requires data to assess and understand the level of care provided, allowing initiatives to maximize the quality of care. Service planners need to understand current service provision, how this varies across patient groups, and how future needs may change. People living with diabetes need access to data that allows them to make informed decisions and maximize their care.</p><p>The definition and identification of people with diagnosed diabetes needs to be specified. This will be an iterative process where individuals are identified from existing datasets including the Diabetic RetinaScreen programme, the CDM programme, records of prescriptions dispensed in the community through the primary care reimbursement service (PCRS), and hospital admissions (where diabetes has been identified) through the hospital inpatient enquiry (HIPE) database. As the system matures and incorporates data from local sources such as general practice and laboratory records, this process will evolve.</p><p>Patient and public involvement needs to be embedded in the programme from the earliest stages. There needs to be a clearly defined process for ensuring that people living with diabetes have a real voice in how the data system develops and that any data analysis has a positive and timely impact on their quality of life. This must acknowledge that there is no single perspective, and capturing the range of views and experiences is vital to ensure the support of the people who form the dataset and for whom the data system seeks to create improvement.</p><p>Although the primary constituent datasets are already known, a data discovery and mapping exercise will be required, and the information governance framework to facilitate the shared storage, linkage, analysis, and reporting will need to be created. This will require clearly defining the function of the data system, the scope of analyses to be undertaken, and ensuring appropriate disclosure control measures are in place. Processes to allow the sharing of data need to be incorporated into the framework to ensure the data system can perform its intended functions. To maintain data integrity and provide greatest flexibility to meet currently identified and unanticipated needs, the component datasets contributing to the data system should be stored as regularly updated standalone datasets. Information from each dataset will be pooled to identify individuals with diagnosed diabetes, and an index file will contain their key demographic characteristics, diagnosis information (e.g. type of diabetes) and identifiers to link to specific datasets in the system. A standard suite of data quality checks and data cleaning processes should be developed for each dataset included in the data system<span><sup>5</sup></span>.</p><p>The foundations of the data system are routinely collated national administrative datasets, so there needs to be scope for it to develop over time and with the flexibility to evolve both in terms of inputs (datasets) and outputs (reports, indicators, bespoke analyses). Regional and local information, population, and disease-specific information need to be incorporated in the future.</p><p>There needs to be a scoping exercise to create a consensus on the nature of outputs from the data system. The fundamental principles are that all outputs are tailored to their audience, data are presented with appropriate context, caveats, and interpretation. Policymakers will require summary-level reports that provide evidence on the current epidemiology of diabetes, the care received by people with diabetes, how treatments and outcomes vary, and provide insight into future requirements of the diabetes community. National reports with complementary local summary data/indicators focusing on clearly defined measurable factors will facilitate quality assessment and improvement. There will be a need to create easily accessible reports for lay audiences where findings are distilled into clear messages in non-technical language presented in the wider context with further support signposted. If the data system is to contribute to the generation of new knowledge, it must include a secure way for analysts and researchers to access individual-level data to undertake appropriate statistical analysis and for dissemination through academic routes such as conferences and peer-reviewed journals.</p><p>Clear, knowledgeable and decisive leadership from clinical and data perspectives will be vital for the development and success of the data system. Integration of expertise from these areas, from the beginning should ensure that it can meet the needs of the diabetes community (including healthcare professionals working in diabetes) and encourage confidence in the data processing, analysis and presentation. Part of this role will be to manage expectations of the diabetes clinical community and among people with diabetes of the scope and capability of the data system. Resources of this nature take time to evolve into comprehensive datasets that can provide a comprehensive picture of care and outcomes. They also need to have dedicated long-term resources and staff allocated and firmly embedded within the core health service rather than perceived to be an ‘add-on’ to clinical care. The Diabetes Data System aims to be one of the exemplars for other chronic diseases in Ireland.</p><p>Outputs from the diabetes data system may highlight variation in care and outcomes which will require careful interpretation. The process of assessing, questioning and action planning should not be under-estimated. Ireland does not have a tradition of providing dashboards to diabetes clinicians or people living with diabetes as a way of motivating them to focus on certain aspects of their practice (or behavior). It is therefore vital that there is support in the interpretation of the outputs from the data system for clinical and patient communities. This must include insight into how the demographic and socio-economic characteristics of individuals with diabetes are (or are not) associated with outcomes. As the foundation of the data system is nationally collated administrative datasets the production of reports and summary measures for and relevant to local health systems creates a circle of feedback to the origins of the data. The accuracy and quality of the data being input need to be reflected in the outputs from the data system. There also needs to be an understanding that timely real-world data of the sort to be created in the data system rarely provides neat and clear cut ‘answers’ to simple questions. In fact, analysis often leads to more questions being asked as people consider the nuances behind and implications of summary figures. Guidance on unpicking the implications of the data and how to navigate service improvement will be essential to the acceptance and success of the data system.</p><p>As the consortium leading this work has evolved organically, it benefits from strong support from senior leaders in clinical, academic, and patient organizations. However, the scale and scope of the task are sizeable. The Irish health system needs a standardized approach to the generation of data systems for diabetes and other chronic conditions. In today's world, data is more readily available, and it is incumbent on us to use data to improve population health. In September 2024, at the time of the Annual Meeting of the European Association for the Study of Diabetes, the European Diabetes Forum (a pan European non-profit multi-stakeholder organization advocating for the translation of research into policy) held a workshop on diabetes registries. Many of the (12–15) national or sub-national registries represented at the workshop had years (or decades) of experience in leveraging change in policy and practice through outputs from robust chronic disease data systems. Ireland was represented at the workshop, and the ambition (described in this article) to establish a diabetes data system for collating, analyzing, and using existing administrative and clinical data to improve the quality of diabetes care for children and adults was acknowledged. Just like the St Vincent Declaration in the 1990s<span><sup>6</sup></span>, this call to action to streamline and harmonize diabetes data systems across Europe should be a motivator to the Health Service Executive and partner organizations to learn from others, harness the impending legislation around an EU Data Space, and improve the lives of people living with diabetes in Ireland.</p>","PeriodicalId":51250,"journal":{"name":"Journal of Diabetes Investigation","volume":"16 8","pages":"1367-1370"},"PeriodicalIF":3.0000,"publicationDate":"2025-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jdi.70080","citationCount":"0","resultStr":"{\"title\":\"The need for a comprehensive diabetes data system in Ireland\",\"authors\":\"Naomi Holman, Claire M. Buckley, Lisa Devine, Kate Gajewska, Sean F. Dinneen, the Chronic Disease Data System Consortium\",\"doi\":\"10.1111/jdi.70080\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The primary purpose of healthcare systems is to prevent and treat disease. The mainstay of this is direct patient clinical care, but the system needs to be supported by reliable and timely data to function in an evidence-based and responsive way<span><sup>1</sup></span>. Many health systems around the globe have a rich tradition of using data to inform and improve care processes<span><sup>2-4</sup></span>. In Ireland, there is currently no single source of data that can reliably report the number of people living with diabetes and no collation of records that provides an overview of the care received and outcomes experienced by people living with diabetes. A dual payer (public/private) system has led to diverse models of care, with a substantial proportion of diabetes care being provided privately by general practitioners. Historically, the lack of a unique identifier makes linkage of (clinical and administrative) data systems challenging. Many questions remain unanswered, and the scope to improve services and health-services planning is hindered without mechanisms to monitor change. Issues of equity and equality remain hidden, and the perspectives of people within the health service on the characteristics and outcomes of people living with diabetes cannot be substantiated by data.</p><p>Without a comprehensive data system, there is no scope to verify (or disprove) perceptions and changes to services that may be made with limited data to support their evaluation; plans are not evidence-based, and data to prioritize and shape policymaking are lacking.</p><p>Currently, aspects of diabetes care are captured in several national administrative datasets, including records of prescriptions dispensed by community pharmacies, publicly funded hospital admissions, Chronic Disease Management (CDM) programme returns by General Practitioners, Diabetic RetinaScreen, and civil death registrations. The combination of public and private care provision in the Irish health service (Figure 1) means that coverage of the datasets is not always universal. Data analysis is limited by a lack of governance, infrastructure, and public engagement that facilitates continuous networked dataset linkage. A national individual health identifier (IHI) has been created, but full implementation requires further legislation. Additionally, some crucial data on the care and outcomes of people with diabetes, such as laboratory tests, anthropometric measures, and lifestyle risk factors, are held in local or sub-national systems, which vary in their compatibility. The need for a diabetes data system has been consistently identified and has the support of the Department of Health, the Health Service Executive (HSE), Diabetes Ireland (national patient organization) and academic organizations. With early funding allocated and posts being filled in 2025, processes are being established to provide clinical leadership, programme management, data management, analysis, and reporting functions.</p><p>To address the gap in data on diabetes care in Ireland, the HSE initiated a programme of work to create a diabetes data system. It will collate administrative data currently used within the health system to identify people with diagnosed diabetes and document their healthcare delivery and outcomes. It aims to be an exemplar that can be applied to other chronic diseases (Figure 2).</p><p>By utilizing existing datasets, the diabetes data system will minimize the burden for clinical staff. It will include the scope to assess the incidence and prevalence of diabetes, the level and variation in care received by people with diabetes, leading to an understanding of equity and equality in healthcare. It will become dynamic by supporting service activity metrics, quality assessment/awareness, improvement of services to enable planning, monitoring, and evaluation, and the generation of new knowledge through scientific methodologies. As the role of real-world data in academic research grows, the data system will provide a rich dataset to explore the epidemiology and health economics of diabetes. In the long term, there is an aspiration of becoming a learning health system moving toward a real-time clinical and administrative data system accessible at the point of clinical care.</p><p>The journey from concept to a fully functioning data system will take many steps. A governance structure is needed to implement and oversee the work programme. The formal structure should include a senior leadership group that sets, guides, and monitors the strategic direction of the health service. An implementation group is required that will focus on the delivery of the data system; appropriate analysis and engagement with the diabetes community is also needed. At all levels, the governance system should be able to make decisions, solve problems, maintain support for the development of the data system, and ensure it meets its specified functions. As described in Figure 2, the function of the data system will vary across user groups. The clinical community requires data to assess and understand the level of care provided, allowing initiatives to maximize the quality of care. Service planners need to understand current service provision, how this varies across patient groups, and how future needs may change. People living with diabetes need access to data that allows them to make informed decisions and maximize their care.</p><p>The definition and identification of people with diagnosed diabetes needs to be specified. This will be an iterative process where individuals are identified from existing datasets including the Diabetic RetinaScreen programme, the CDM programme, records of prescriptions dispensed in the community through the primary care reimbursement service (PCRS), and hospital admissions (where diabetes has been identified) through the hospital inpatient enquiry (HIPE) database. As the system matures and incorporates data from local sources such as general practice and laboratory records, this process will evolve.</p><p>Patient and public involvement needs to be embedded in the programme from the earliest stages. There needs to be a clearly defined process for ensuring that people living with diabetes have a real voice in how the data system develops and that any data analysis has a positive and timely impact on their quality of life. This must acknowledge that there is no single perspective, and capturing the range of views and experiences is vital to ensure the support of the people who form the dataset and for whom the data system seeks to create improvement.</p><p>Although the primary constituent datasets are already known, a data discovery and mapping exercise will be required, and the information governance framework to facilitate the shared storage, linkage, analysis, and reporting will need to be created. This will require clearly defining the function of the data system, the scope of analyses to be undertaken, and ensuring appropriate disclosure control measures are in place. Processes to allow the sharing of data need to be incorporated into the framework to ensure the data system can perform its intended functions. To maintain data integrity and provide greatest flexibility to meet currently identified and unanticipated needs, the component datasets contributing to the data system should be stored as regularly updated standalone datasets. Information from each dataset will be pooled to identify individuals with diagnosed diabetes, and an index file will contain their key demographic characteristics, diagnosis information (e.g. type of diabetes) and identifiers to link to specific datasets in the system. A standard suite of data quality checks and data cleaning processes should be developed for each dataset included in the data system<span><sup>5</sup></span>.</p><p>The foundations of the data system are routinely collated national administrative datasets, so there needs to be scope for it to develop over time and with the flexibility to evolve both in terms of inputs (datasets) and outputs (reports, indicators, bespoke analyses). Regional and local information, population, and disease-specific information need to be incorporated in the future.</p><p>There needs to be a scoping exercise to create a consensus on the nature of outputs from the data system. The fundamental principles are that all outputs are tailored to their audience, data are presented with appropriate context, caveats, and interpretation. Policymakers will require summary-level reports that provide evidence on the current epidemiology of diabetes, the care received by people with diabetes, how treatments and outcomes vary, and provide insight into future requirements of the diabetes community. National reports with complementary local summary data/indicators focusing on clearly defined measurable factors will facilitate quality assessment and improvement. There will be a need to create easily accessible reports for lay audiences where findings are distilled into clear messages in non-technical language presented in the wider context with further support signposted. If the data system is to contribute to the generation of new knowledge, it must include a secure way for analysts and researchers to access individual-level data to undertake appropriate statistical analysis and for dissemination through academic routes such as conferences and peer-reviewed journals.</p><p>Clear, knowledgeable and decisive leadership from clinical and data perspectives will be vital for the development and success of the data system. Integration of expertise from these areas, from the beginning should ensure that it can meet the needs of the diabetes community (including healthcare professionals working in diabetes) and encourage confidence in the data processing, analysis and presentation. Part of this role will be to manage expectations of the diabetes clinical community and among people with diabetes of the scope and capability of the data system. Resources of this nature take time to evolve into comprehensive datasets that can provide a comprehensive picture of care and outcomes. They also need to have dedicated long-term resources and staff allocated and firmly embedded within the core health service rather than perceived to be an ‘add-on’ to clinical care. The Diabetes Data System aims to be one of the exemplars for other chronic diseases in Ireland.</p><p>Outputs from the diabetes data system may highlight variation in care and outcomes which will require careful interpretation. The process of assessing, questioning and action planning should not be under-estimated. Ireland does not have a tradition of providing dashboards to diabetes clinicians or people living with diabetes as a way of motivating them to focus on certain aspects of their practice (or behavior). It is therefore vital that there is support in the interpretation of the outputs from the data system for clinical and patient communities. This must include insight into how the demographic and socio-economic characteristics of individuals with diabetes are (or are not) associated with outcomes. As the foundation of the data system is nationally collated administrative datasets the production of reports and summary measures for and relevant to local health systems creates a circle of feedback to the origins of the data. The accuracy and quality of the data being input need to be reflected in the outputs from the data system. There also needs to be an understanding that timely real-world data of the sort to be created in the data system rarely provides neat and clear cut ‘answers’ to simple questions. In fact, analysis often leads to more questions being asked as people consider the nuances behind and implications of summary figures. Guidance on unpicking the implications of the data and how to navigate service improvement will be essential to the acceptance and success of the data system.</p><p>As the consortium leading this work has evolved organically, it benefits from strong support from senior leaders in clinical, academic, and patient organizations. However, the scale and scope of the task are sizeable. The Irish health system needs a standardized approach to the generation of data systems for diabetes and other chronic conditions. In today's world, data is more readily available, and it is incumbent on us to use data to improve population health. In September 2024, at the time of the Annual Meeting of the European Association for the Study of Diabetes, the European Diabetes Forum (a pan European non-profit multi-stakeholder organization advocating for the translation of research into policy) held a workshop on diabetes registries. Many of the (12–15) national or sub-national registries represented at the workshop had years (or decades) of experience in leveraging change in policy and practice through outputs from robust chronic disease data systems. Ireland was represented at the workshop, and the ambition (described in this article) to establish a diabetes data system for collating, analyzing, and using existing administrative and clinical data to improve the quality of diabetes care for children and adults was acknowledged. Just like the St Vincent Declaration in the 1990s<span><sup>6</sup></span>, this call to action to streamline and harmonize diabetes data systems across Europe should be a motivator to the Health Service Executive and partner organizations to learn from others, harness the impending legislation around an EU Data Space, and improve the lives of people living with diabetes in Ireland.</p>\",\"PeriodicalId\":51250,\"journal\":{\"name\":\"Journal of Diabetes Investigation\",\"volume\":\"16 8\",\"pages\":\"1367-1370\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-05-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jdi.70080\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Diabetes Investigation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jdi.70080\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Diabetes Investigation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jdi.70080","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
临床社区需要数据来评估和了解所提供的护理水平,从而使倡议能够最大限度地提高护理质量。服务规划者需要了解当前的服务供应,不同患者群体之间的差异,以及未来需求可能发生的变化。糖尿病患者需要获得数据,使他们能够做出明智的决定并最大限度地获得治疗。确诊糖尿病患者的定义和鉴定需要明确。这将是一个反复的过程,从现有的数据集中识别个体,包括糖尿病视网膜筛查项目、CDM项目、通过初级保健报销服务(PCRS)在社区分配的处方记录,以及通过医院住院咨询(HIPE)数据库确定的住院(糖尿病患者)。随着系统的成熟,并纳入当地来源的数据,如一般做法和实验室记录,这一过程将不断发展。病人和公众的参与需要从最初阶段就融入到规划中。需要有一个明确定义的过程,以确保糖尿病患者对数据系统的发展有真正的发言权,并确保任何数据分析对他们的生活质量产生积极和及时的影响。这必须承认,没有单一的视角,捕捉各种观点和经验对于确保数据集的形成者和数据系统寻求改进的对象的支持至关重要。虽然已经知道了主要的组成数据集,但是还需要进行数据发现和映射,并且还需要创建促进共享存储、链接、分析和报告的信息治理框架。这将需要明确界定数据系统的功能、要进行的分析范围,并确保有适当的披露控制措施。允许共享数据的过程需要合并到框架中,以确保数据系统能够执行其预期的功能。为了保持数据的完整性,并提供最大的灵活性,以满足当前确定的和未预料到的需求,对数据系统有贡献的组件数据集应该作为定期更新的独立数据集存储。来自每个数据集的信息将被汇集起来,以识别诊断为糖尿病的个体,索引文件将包含他们的关键人口统计学特征、诊断信息(例如糖尿病类型)和标识符,以链接到系统中的特定数据集。应该为数据系统中包含的每个数据集开发一套标准的数据质量检查和数据清理流程5。数据系统的基础是定期整理的国家行政数据集,因此需要有一定的发展空间,使其在投入(数据集)和产出(报告、指标、定制分析)方面都能灵活发展。未来需要纳入区域和地方信息、人口和特定疾病信息。需要进行范围界定工作,以便就数据系统输出的性质达成共识。基本原则是,所有产出都是针对其受众量身定制的,数据呈现时要有适当的背景、说明和解释。决策者将要求概要级报告提供有关当前糖尿病流行病学、糖尿病患者接受的护理、治疗和结果如何变化的证据,并提供对糖尿病社区未来需求的见解。国家报告加上补充的地方摘要数据/指标,侧重于明确界定的可衡量因素,将有助于质量评估和改进。将需要为外行读者编写易于获取的报告,其中的调查结果将被提炼成在更广泛的背景下以非技术语言呈现的明确信息,并附有进一步支持的路标。如果数据系统要对新知识的产生作出贡献,它必须包括一种安全的方式,使分析人员和研究人员能够访问个人层面的数据,进行适当的统计分析,并通过会议和同行评议期刊等学术途径进行传播。从临床和数据的角度来看,清晰、知识渊博和果断的领导对数据系统的发展和成功至关重要。从一开始就整合这些领域的专业知识,应确保它能够满足糖尿病社区(包括从事糖尿病工作的医疗保健专业人员)的需求,并鼓励对数据处理、分析和呈现的信心。这个角色的一部分将是管理糖尿病临床社区和糖尿病患者对数据系统的范围和能力的期望。 这种性质的资源需要时间才能演变成全面的数据集,从而提供全面的护理和结果。它们还需要有专门的长期资源和人员分配,并牢固地嵌入核心卫生服务,而不是被视为临床护理的“附加”。糖尿病数据系统旨在成为爱尔兰其他慢性疾病的典范之一。糖尿病数据系统的输出可能会突出护理和结果的差异,这需要仔细解释。不应低估评估、质疑和行动规划的过程。爱尔兰没有向糖尿病临床医生或糖尿病患者提供仪表板的传统,这是一种激励他们专注于实践(或行为)某些方面的方式。因此,对临床和患者社区数据系统输出的解释提供支持是至关重要的。这必须包括洞察糖尿病患者的人口统计学和社会经济特征如何与结果相关(或不相关)。由于数据系统的基础是国家整理的行政数据集,因此为地方卫生系统编写报告和汇总措施并与之相关,形成了对数据来源的反馈循环。输入数据的准确性和质量需要反映在数据系统的输出中。还需要理解的是,在数据系统中创建的实时真实数据很少能为简单的问题提供简洁明了的“答案”。事实上,当人们考虑汇总数据背后的细微差别和含义时,分析往往会导致更多的问题被提出。对数据系统的接受和成功来说,提供有关分析数据含义和如何改进服务的指导是必不可少的。随着领导这项工作的联盟有机地发展,它从临床、学术和患者组织的高级领导人的大力支持中受益。然而,这项任务的规模和范围是相当大的。爱尔兰卫生系统需要一种标准化的方法来生成糖尿病和其他慢性疾病的数据系统。在当今世界,数据更容易获得,我们有责任利用数据改善人口健康。2024年9月,在欧洲糖尿病研究协会年会期间,欧洲糖尿病论坛(一个倡导将研究转化为政策的泛欧洲非营利性多方利益相关者组织)举办了一次关于糖尿病登记的研讨会。出席研讨会的许多(12-15个)国家或国家以下各级登记处都有多年(或数十年)的经验,通过强大的慢性病数据系统的产出来利用政策和实践的变化。爱尔兰派代表参加了研讨会,并承认了建立糖尿病数据系统的雄心(在本文中描述),该系统用于整理、分析和使用现有的行政和临床数据,以提高儿童和成人糖尿病护理的质量。就像20世纪90年代的《圣文森特宣言》(St Vincent Declaration)一样,这项旨在简化和协调整个欧洲糖尿病数据系统的行动呼吁,应该激励卫生服务行政部门和合作伙伴组织向其他机构学习,利用欧盟数据空间(EU data Space)即将出台的立法,改善爱尔兰糖尿病患者的生活。
The need for a comprehensive diabetes data system in Ireland
The primary purpose of healthcare systems is to prevent and treat disease. The mainstay of this is direct patient clinical care, but the system needs to be supported by reliable and timely data to function in an evidence-based and responsive way1. Many health systems around the globe have a rich tradition of using data to inform and improve care processes2-4. In Ireland, there is currently no single source of data that can reliably report the number of people living with diabetes and no collation of records that provides an overview of the care received and outcomes experienced by people living with diabetes. A dual payer (public/private) system has led to diverse models of care, with a substantial proportion of diabetes care being provided privately by general practitioners. Historically, the lack of a unique identifier makes linkage of (clinical and administrative) data systems challenging. Many questions remain unanswered, and the scope to improve services and health-services planning is hindered without mechanisms to monitor change. Issues of equity and equality remain hidden, and the perspectives of people within the health service on the characteristics and outcomes of people living with diabetes cannot be substantiated by data.
Without a comprehensive data system, there is no scope to verify (or disprove) perceptions and changes to services that may be made with limited data to support their evaluation; plans are not evidence-based, and data to prioritize and shape policymaking are lacking.
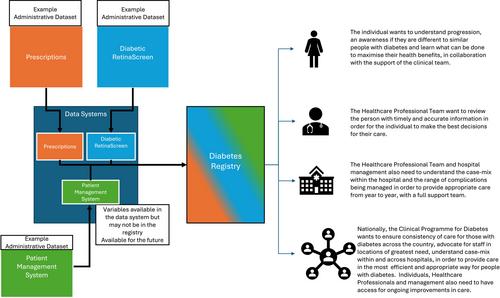
Currently, aspects of diabetes care are captured in several national administrative datasets, including records of prescriptions dispensed by community pharmacies, publicly funded hospital admissions, Chronic Disease Management (CDM) programme returns by General Practitioners, Diabetic RetinaScreen, and civil death registrations. The combination of public and private care provision in the Irish health service (Figure 1) means that coverage of the datasets is not always universal. Data analysis is limited by a lack of governance, infrastructure, and public engagement that facilitates continuous networked dataset linkage. A national individual health identifier (IHI) has been created, but full implementation requires further legislation. Additionally, some crucial data on the care and outcomes of people with diabetes, such as laboratory tests, anthropometric measures, and lifestyle risk factors, are held in local or sub-national systems, which vary in their compatibility. The need for a diabetes data system has been consistently identified and has the support of the Department of Health, the Health Service Executive (HSE), Diabetes Ireland (national patient organization) and academic organizations. With early funding allocated and posts being filled in 2025, processes are being established to provide clinical leadership, programme management, data management, analysis, and reporting functions.
To address the gap in data on diabetes care in Ireland, the HSE initiated a programme of work to create a diabetes data system. It will collate administrative data currently used within the health system to identify people with diagnosed diabetes and document their healthcare delivery and outcomes. It aims to be an exemplar that can be applied to other chronic diseases (Figure 2).
By utilizing existing datasets, the diabetes data system will minimize the burden for clinical staff. It will include the scope to assess the incidence and prevalence of diabetes, the level and variation in care received by people with diabetes, leading to an understanding of equity and equality in healthcare. It will become dynamic by supporting service activity metrics, quality assessment/awareness, improvement of services to enable planning, monitoring, and evaluation, and the generation of new knowledge through scientific methodologies. As the role of real-world data in academic research grows, the data system will provide a rich dataset to explore the epidemiology and health economics of diabetes. In the long term, there is an aspiration of becoming a learning health system moving toward a real-time clinical and administrative data system accessible at the point of clinical care.
The journey from concept to a fully functioning data system will take many steps. A governance structure is needed to implement and oversee the work programme. The formal structure should include a senior leadership group that sets, guides, and monitors the strategic direction of the health service. An implementation group is required that will focus on the delivery of the data system; appropriate analysis and engagement with the diabetes community is also needed. At all levels, the governance system should be able to make decisions, solve problems, maintain support for the development of the data system, and ensure it meets its specified functions. As described in Figure 2, the function of the data system will vary across user groups. The clinical community requires data to assess and understand the level of care provided, allowing initiatives to maximize the quality of care. Service planners need to understand current service provision, how this varies across patient groups, and how future needs may change. People living with diabetes need access to data that allows them to make informed decisions and maximize their care.
The definition and identification of people with diagnosed diabetes needs to be specified. This will be an iterative process where individuals are identified from existing datasets including the Diabetic RetinaScreen programme, the CDM programme, records of prescriptions dispensed in the community through the primary care reimbursement service (PCRS), and hospital admissions (where diabetes has been identified) through the hospital inpatient enquiry (HIPE) database. As the system matures and incorporates data from local sources such as general practice and laboratory records, this process will evolve.
Patient and public involvement needs to be embedded in the programme from the earliest stages. There needs to be a clearly defined process for ensuring that people living with diabetes have a real voice in how the data system develops and that any data analysis has a positive and timely impact on their quality of life. This must acknowledge that there is no single perspective, and capturing the range of views and experiences is vital to ensure the support of the people who form the dataset and for whom the data system seeks to create improvement.
Although the primary constituent datasets are already known, a data discovery and mapping exercise will be required, and the information governance framework to facilitate the shared storage, linkage, analysis, and reporting will need to be created. This will require clearly defining the function of the data system, the scope of analyses to be undertaken, and ensuring appropriate disclosure control measures are in place. Processes to allow the sharing of data need to be incorporated into the framework to ensure the data system can perform its intended functions. To maintain data integrity and provide greatest flexibility to meet currently identified and unanticipated needs, the component datasets contributing to the data system should be stored as regularly updated standalone datasets. Information from each dataset will be pooled to identify individuals with diagnosed diabetes, and an index file will contain their key demographic characteristics, diagnosis information (e.g. type of diabetes) and identifiers to link to specific datasets in the system. A standard suite of data quality checks and data cleaning processes should be developed for each dataset included in the data system5.
The foundations of the data system are routinely collated national administrative datasets, so there needs to be scope for it to develop over time and with the flexibility to evolve both in terms of inputs (datasets) and outputs (reports, indicators, bespoke analyses). Regional and local information, population, and disease-specific information need to be incorporated in the future.
There needs to be a scoping exercise to create a consensus on the nature of outputs from the data system. The fundamental principles are that all outputs are tailored to their audience, data are presented with appropriate context, caveats, and interpretation. Policymakers will require summary-level reports that provide evidence on the current epidemiology of diabetes, the care received by people with diabetes, how treatments and outcomes vary, and provide insight into future requirements of the diabetes community. National reports with complementary local summary data/indicators focusing on clearly defined measurable factors will facilitate quality assessment and improvement. There will be a need to create easily accessible reports for lay audiences where findings are distilled into clear messages in non-technical language presented in the wider context with further support signposted. If the data system is to contribute to the generation of new knowledge, it must include a secure way for analysts and researchers to access individual-level data to undertake appropriate statistical analysis and for dissemination through academic routes such as conferences and peer-reviewed journals.
Clear, knowledgeable and decisive leadership from clinical and data perspectives will be vital for the development and success of the data system. Integration of expertise from these areas, from the beginning should ensure that it can meet the needs of the diabetes community (including healthcare professionals working in diabetes) and encourage confidence in the data processing, analysis and presentation. Part of this role will be to manage expectations of the diabetes clinical community and among people with diabetes of the scope and capability of the data system. Resources of this nature take time to evolve into comprehensive datasets that can provide a comprehensive picture of care and outcomes. They also need to have dedicated long-term resources and staff allocated and firmly embedded within the core health service rather than perceived to be an ‘add-on’ to clinical care. The Diabetes Data System aims to be one of the exemplars for other chronic diseases in Ireland.
Outputs from the diabetes data system may highlight variation in care and outcomes which will require careful interpretation. The process of assessing, questioning and action planning should not be under-estimated. Ireland does not have a tradition of providing dashboards to diabetes clinicians or people living with diabetes as a way of motivating them to focus on certain aspects of their practice (or behavior). It is therefore vital that there is support in the interpretation of the outputs from the data system for clinical and patient communities. This must include insight into how the demographic and socio-economic characteristics of individuals with diabetes are (or are not) associated with outcomes. As the foundation of the data system is nationally collated administrative datasets the production of reports and summary measures for and relevant to local health systems creates a circle of feedback to the origins of the data. The accuracy and quality of the data being input need to be reflected in the outputs from the data system. There also needs to be an understanding that timely real-world data of the sort to be created in the data system rarely provides neat and clear cut ‘answers’ to simple questions. In fact, analysis often leads to more questions being asked as people consider the nuances behind and implications of summary figures. Guidance on unpicking the implications of the data and how to navigate service improvement will be essential to the acceptance and success of the data system.
As the consortium leading this work has evolved organically, it benefits from strong support from senior leaders in clinical, academic, and patient organizations. However, the scale and scope of the task are sizeable. The Irish health system needs a standardized approach to the generation of data systems for diabetes and other chronic conditions. In today's world, data is more readily available, and it is incumbent on us to use data to improve population health. In September 2024, at the time of the Annual Meeting of the European Association for the Study of Diabetes, the European Diabetes Forum (a pan European non-profit multi-stakeholder organization advocating for the translation of research into policy) held a workshop on diabetes registries. Many of the (12–15) national or sub-national registries represented at the workshop had years (or decades) of experience in leveraging change in policy and practice through outputs from robust chronic disease data systems. Ireland was represented at the workshop, and the ambition (described in this article) to establish a diabetes data system for collating, analyzing, and using existing administrative and clinical data to improve the quality of diabetes care for children and adults was acknowledged. Just like the St Vincent Declaration in the 1990s6, this call to action to streamline and harmonize diabetes data systems across Europe should be a motivator to the Health Service Executive and partner organizations to learn from others, harness the impending legislation around an EU Data Space, and improve the lives of people living with diabetes in Ireland.
期刊介绍:
Journal of Diabetes Investigation is your core diabetes journal from Asia; the official journal of the Asian Association for the Study of Diabetes (AASD). The journal publishes original research, country reports, commentaries, reviews, mini-reviews, case reports, letters, as well as editorials and news. Embracing clinical and experimental research in diabetes and related areas, the Journal of Diabetes Investigation includes aspects of prevention, treatment, as well as molecular aspects and pathophysiology. Translational research focused on the exchange of ideas between clinicians and researchers is also welcome. Journal of Diabetes Investigation is indexed by Science Citation Index Expanded (SCIE).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


