{"title":"接受化疗的儿童癌症幸存者控制卵巢刺激保存卵母细胞。","authors":"Moran Shapira, Dror Meirow, Dani Raved, Leyla Levy, Noah Gruber, Dalit Modan-Moses, Raoul Orvieto, Myriam Safrai","doi":"10.1093/hropen/hoaf023","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>What are the outcomes of controlled ovarian stimulation (COS) in childhood cancer survivors (CCS) undergoing fertility preservation (FP) after cancer treatment?</p><p><strong>Summary answer: </strong>CCS who have undergone chemotherapy often show poor outcomes with COS and may need multiple cycles to achieve an adequate number of oocytes for future pregnancy.</p><p><strong>What is known already: </strong>Up to 65% of CCS experience infertility from gonadotoxic treatments. Although it is ideal to consider FP at diagnosis, age and oncological factors often limit this option. After recovery, pubescent survivors, especially those who could not preserve fertility earlier, may be offered oocyte cryopreservation.</p><p><strong>Study design size duration: </strong>A retrospective study including 20 CCS who underwent COS for oocyte storage between 2015 and 2022.</p><p><strong>Participants/materials setting methods: </strong>This study involved young CCS who had been previously treated with chemotherapy and were evaluated at an FP center in a tertiary medical center. CCS were encouraged to pursue endocrine surveillance after recovering from cancer and were offered oocyte storage in case diminished ovarian reserve was evident, as dictated by elevated basal FSH (>10 IU/l), decreased anti-Müllerian hormone (AMH; <25th percentile for age), or low antral follicle count (<7).</p><p><strong>Main results and the role of chance: </strong>Mean age at cancer diagnosis was 13.24 ± 5.6 years. Seventeen patients (85%) had been treated with alkylating agents, with five receiving cumulative doses greater than 4000 mg/m<sup>2</sup>. At the time of FP, a median of 4.25 years after cancer diagnosis, the mean age of patients was 20.6 ± 3.56 years. Mean Day 3 FSH levels were 9.26 ± 3.4 IU/l, and 12 patients had AMH levels below 1 ng/ml. The first stimulation cycle lasted 9.4 ± 2.1 days, with a mean gonadotropin dose of 3246 ± 1057 IU and a median peak estradiol (E2) level of 3733 pmol/ml (IQR 1424-6796). The median number of oocytes retrieved in the first stimulation cycle was 5.5, with a median of four mature oocytes. By the end of the FP process, which involved 1-7 cycles per patient, the median number of oocytes stored was 13.5 (IQR 3.5-18.5). Twelve patients managed to store more than 10 oocytes.</p><p><strong>Limitations reasons for caution: </strong>The study is exploratory in its nature, limited by its small sample size and its retrospective design.</p><p><strong>Wider implications of the findings: </strong>Oocyte storage is feasible yet limited in young CCS. Despite their young age at the time of FP, CCS who have undergone chemotherapy often show poor outcomes with COS. Ongoing reproductive monitoring after recovery is crucial to identify those who would benefit from FP following cancer treatment.</p><p><strong>Study funding/competing interests: </strong>The Fertility Preservation Unit funds (Sheba Medical Center) were used to support the authors throughout the study period and manuscript preparation. None of the authors declare any conflicts of interest.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2025 2","pages":"hoaf023"},"PeriodicalIF":11.1000,"publicationDate":"2025-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12122208/pdf/","citationCount":"0","resultStr":"{\"title\":\"Controlled ovarian stimulation for oocyte preservation in childhood cancer survivors who have undergone chemotherapy.\",\"authors\":\"Moran Shapira, Dror Meirow, Dani Raved, Leyla Levy, Noah Gruber, Dalit Modan-Moses, Raoul Orvieto, Myriam Safrai\",\"doi\":\"10.1093/hropen/hoaf023\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study question: </strong>What are the outcomes of controlled ovarian stimulation (COS) in childhood cancer survivors (CCS) undergoing fertility preservation (FP) after cancer treatment?</p><p><strong>Summary answer: </strong>CCS who have undergone chemotherapy often show poor outcomes with COS and may need multiple cycles to achieve an adequate number of oocytes for future pregnancy.</p><p><strong>What is known already: </strong>Up to 65% of CCS experience infertility from gonadotoxic treatments. Although it is ideal to consider FP at diagnosis, age and oncological factors often limit this option. After recovery, pubescent survivors, especially those who could not preserve fertility earlier, may be offered oocyte cryopreservation.</p><p><strong>Study design size duration: </strong>A retrospective study including 20 CCS who underwent COS for oocyte storage between 2015 and 2022.</p><p><strong>Participants/materials setting methods: </strong>This study involved young CCS who had been previously treated with chemotherapy and were evaluated at an FP center in a tertiary medical center. CCS were encouraged to pursue endocrine surveillance after recovering from cancer and were offered oocyte storage in case diminished ovarian reserve was evident, as dictated by elevated basal FSH (>10 IU/l), decreased anti-Müllerian hormone (AMH; <25th percentile for age), or low antral follicle count (<7).</p><p><strong>Main results and the role of chance: </strong>Mean age at cancer diagnosis was 13.24 ± 5.6 years. Seventeen patients (85%) had been treated with alkylating agents, with five receiving cumulative doses greater than 4000 mg/m<sup>2</sup>. At the time of FP, a median of 4.25 years after cancer diagnosis, the mean age of patients was 20.6 ± 3.56 years. Mean Day 3 FSH levels were 9.26 ± 3.4 IU/l, and 12 patients had AMH levels below 1 ng/ml. The first stimulation cycle lasted 9.4 ± 2.1 days, with a mean gonadotropin dose of 3246 ± 1057 IU and a median peak estradiol (E2) level of 3733 pmol/ml (IQR 1424-6796). The median number of oocytes retrieved in the first stimulation cycle was 5.5, with a median of four mature oocytes. By the end of the FP process, which involved 1-7 cycles per patient, the median number of oocytes stored was 13.5 (IQR 3.5-18.5). Twelve patients managed to store more than 10 oocytes.</p><p><strong>Limitations reasons for caution: </strong>The study is exploratory in its nature, limited by its small sample size and its retrospective design.</p><p><strong>Wider implications of the findings: </strong>Oocyte storage is feasible yet limited in young CCS. Despite their young age at the time of FP, CCS who have undergone chemotherapy often show poor outcomes with COS. Ongoing reproductive monitoring after recovery is crucial to identify those who would benefit from FP following cancer treatment.</p><p><strong>Study funding/competing interests: </strong>The Fertility Preservation Unit funds (Sheba Medical Center) were used to support the authors throughout the study period and manuscript preparation. None of the authors declare any conflicts of interest.</p><p><strong>Trial registration number: </strong>N/A.</p>\",\"PeriodicalId\":73264,\"journal\":{\"name\":\"Human reproduction open\",\"volume\":\"2025 2\",\"pages\":\"hoaf023\"},\"PeriodicalIF\":11.1000,\"publicationDate\":\"2025-05-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12122208/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Human reproduction open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/hropen/hoaf023\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoaf023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Controlled ovarian stimulation for oocyte preservation in childhood cancer survivors who have undergone chemotherapy.
Study question: What are the outcomes of controlled ovarian stimulation (COS) in childhood cancer survivors (CCS) undergoing fertility preservation (FP) after cancer treatment?
Summary answer: CCS who have undergone chemotherapy often show poor outcomes with COS and may need multiple cycles to achieve an adequate number of oocytes for future pregnancy.
What is known already: Up to 65% of CCS experience infertility from gonadotoxic treatments. Although it is ideal to consider FP at diagnosis, age and oncological factors often limit this option. After recovery, pubescent survivors, especially those who could not preserve fertility earlier, may be offered oocyte cryopreservation.
Study design size duration: A retrospective study including 20 CCS who underwent COS for oocyte storage between 2015 and 2022.
Participants/materials setting methods: This study involved young CCS who had been previously treated with chemotherapy and were evaluated at an FP center in a tertiary medical center. CCS were encouraged to pursue endocrine surveillance after recovering from cancer and were offered oocyte storage in case diminished ovarian reserve was evident, as dictated by elevated basal FSH (>10 IU/l), decreased anti-Müllerian hormone (AMH; <25th percentile for age), or low antral follicle count (<7).
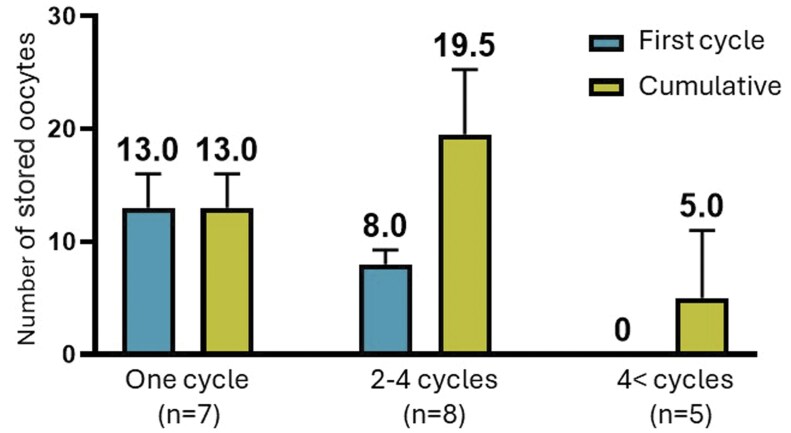
Main results and the role of chance: Mean age at cancer diagnosis was 13.24 ± 5.6 years. Seventeen patients (85%) had been treated with alkylating agents, with five receiving cumulative doses greater than 4000 mg/m2. At the time of FP, a median of 4.25 years after cancer diagnosis, the mean age of patients was 20.6 ± 3.56 years. Mean Day 3 FSH levels were 9.26 ± 3.4 IU/l, and 12 patients had AMH levels below 1 ng/ml. The first stimulation cycle lasted 9.4 ± 2.1 days, with a mean gonadotropin dose of 3246 ± 1057 IU and a median peak estradiol (E2) level of 3733 pmol/ml (IQR 1424-6796). The median number of oocytes retrieved in the first stimulation cycle was 5.5, with a median of four mature oocytes. By the end of the FP process, which involved 1-7 cycles per patient, the median number of oocytes stored was 13.5 (IQR 3.5-18.5). Twelve patients managed to store more than 10 oocytes.
Limitations reasons for caution: The study is exploratory in its nature, limited by its small sample size and its retrospective design.
Wider implications of the findings: Oocyte storage is feasible yet limited in young CCS. Despite their young age at the time of FP, CCS who have undergone chemotherapy often show poor outcomes with COS. Ongoing reproductive monitoring after recovery is crucial to identify those who would benefit from FP following cancer treatment.
Study funding/competing interests: The Fertility Preservation Unit funds (Sheba Medical Center) were used to support the authors throughout the study period and manuscript preparation. None of the authors declare any conflicts of interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


