Andres Rosende, Cesar Romero, Donald J DiPette, Jeffrey Brettler, Patrick Van der Stuyft, Gautam Satheesh, Pablo Perel, Niamh Chapman, Andrew E Moran, Aletta E Schutte, James E Sharman, Vilma Irazola, Mark D Huffman, Norm R C Campbell, Abdul Salam, Fernando Lanas, Antonio Coca, Sebastian Garcia-Zamora, Alejandro Ferreiro, Patricio Lopez-Jaramillo, Jorge Rico-Fontalvo, Emily Ridley, Dean Picone, David Flood, Daniel José Piñeiro, Carolina Neira Ojeda, Gonzalo Rodriguez, Irmgardt A Wellmann, Marcelo Orias, Marcela Rivera, Matías Villatoro Reyes, Oyere Onuma, Shaun Ramroop, Taskeen Khan, Yamile Valdes Gonzalez, Weimar Kunz Sebba Barroso, Frida L Plavnik, Eric Zuniga, Ana María Grassani, Carlos Tajer, Ezequiel Zaidel, Marcos J Marin, Shana Cyr-Philbert, Ignacio Amorin, Miguel Angel Diaz Aguilera, Luiz Bortolotto, Alvaro Avezum, Antonio Luiz P Ribeiro, Sheldon Tobe, Teresa Aumala, Sonia Angell, Pablo Lavados, Sheila Ouriques Martins, Ana Munera Echeverri, Marc G Jaffe, Dorairaj Prabhakaran, Gianfranco Parati, Xin Hua Zhang, Anthony Rodgers, Salim Yusuf, Paul K Whelton, Pedro Ordunez
{"title":"在初级卫生机构中整合高血压和心血管-肾脏-代谢护理的候选干预措施:HEARTS 2.0阶段1","authors":"Andres Rosende, Cesar Romero, Donald J DiPette, Jeffrey Brettler, Patrick Van der Stuyft, Gautam Satheesh, Pablo Perel, Niamh Chapman, Andrew E Moran, Aletta E Schutte, James E Sharman, Vilma Irazola, Mark D Huffman, Norm R C Campbell, Abdul Salam, Fernando Lanas, Antonio Coca, Sebastian Garcia-Zamora, Alejandro Ferreiro, Patricio Lopez-Jaramillo, Jorge Rico-Fontalvo, Emily Ridley, Dean Picone, David Flood, Daniel José Piñeiro, Carolina Neira Ojeda, Gonzalo Rodriguez, Irmgardt A Wellmann, Marcelo Orias, Marcela Rivera, Matías Villatoro Reyes, Oyere Onuma, Shaun Ramroop, Taskeen Khan, Yamile Valdes Gonzalez, Weimar Kunz Sebba Barroso, Frida L Plavnik, Eric Zuniga, Ana María Grassani, Carlos Tajer, Ezequiel Zaidel, Marcos J Marin, Shana Cyr-Philbert, Ignacio Amorin, Miguel Angel Diaz Aguilera, Luiz Bortolotto, Alvaro Avezum, Antonio Luiz P Ribeiro, Sheldon Tobe, Teresa Aumala, Sonia Angell, Pablo Lavados, Sheila Ouriques Martins, Ana Munera Echeverri, Marc G Jaffe, Dorairaj Prabhakaran, Gianfranco Parati, Xin Hua Zhang, Anthony Rodgers, Salim Yusuf, Paul K Whelton, Pedro Ordunez","doi":"10.5334/gh.1428","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>HEARTS in the Americas is the regional adaptation of the WHO Global HEARTS Initiative, aimed at helping countries enhance hypertension and cardiovascular disease (CVD) risk management in primary care settings. Its core implementation tool, the HEARTS Clinical Pathway, has been adopted by 28 countries. To improve the care of hypertension, diabetes, and chronic kidney disease (CKD), HEARTS 2.0 was developed as a three-phase process to integrate evidence-based interventions into a unified care pathway, ensuring consistency across fragmented guidelines. This paper focuses on Phase 1, highlighting targeted interventions to improve and update the HEARTS Clinical Pathway.</p><p><strong>Methods: </strong>First, the coordinating group defined the project's scope, objectives, principles, methodological framework, and tools. Second, international experts from different disciplines proposed interventions to enhance the HEARTS Clinical Pathway. Third, the coordinating group harmonized these proposals into unique interventions. Fourth, experts appraised the appropriateness of the proposed interventions on a 1-to-9 scale using the adapted RAND/UCLA Appropriateness Method. Finally, interventions with a median score above 6 were deemed appropriate and selected as candidates to enhance the HEARTS Clinical Pathway.</p><p><strong>Results: </strong>Building on the existing HEARTS Clinical Pathway, 45 unique interventions were selected, including community-based screening, early detection and management of risk factors, lower blood pressure thresholds for diagnosing hypertension in high-CVD-risk patients, reinforcement of single-pill combination therapy, inclusion of sodium-glucose cotransporter-2 inhibitors for patients with diabetes, CKD, or heart failure, expanded roles for non-physician health workers in team-based care, and strengthened clinical documentation, monitoring, and evaluation.</p><p><strong>Conclusion: </strong>HEARTS 2.0 Phase 1 identifies key interventions to integrate and improve hypertension and cardiovascular-kidney-metabolic care within primary care, enabling their seamless incorporation into a unified and effective clinical pathway. This process will inform an update to the HEARTS Clinical Pathway, optimizing resources, reducing care fragmentation, improving care delivery, and advancing health equity, thereby supporting global efforts to combat the leading causes of death and disability.</p>","PeriodicalId":56018,"journal":{"name":"Global Heart","volume":"20 1","pages":"45"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12124280/pdf/","citationCount":"0","resultStr":"{\"title\":\"Candidate Interventions for Integrating Hypertension and Cardiovascular-Kidney-Metabolic Care in Primary Health Settings: HEARTS 2.0 Phase 1.\",\"authors\":\"Andres Rosende, Cesar Romero, Donald J DiPette, Jeffrey Brettler, Patrick Van der Stuyft, Gautam Satheesh, Pablo Perel, Niamh Chapman, Andrew E Moran, Aletta E Schutte, James E Sharman, Vilma Irazola, Mark D Huffman, Norm R C Campbell, Abdul Salam, Fernando Lanas, Antonio Coca, Sebastian Garcia-Zamora, Alejandro Ferreiro, Patricio Lopez-Jaramillo, Jorge Rico-Fontalvo, Emily Ridley, Dean Picone, David Flood, Daniel José Piñeiro, Carolina Neira Ojeda, Gonzalo Rodriguez, Irmgardt A Wellmann, Marcelo Orias, Marcela Rivera, Matías Villatoro Reyes, Oyere Onuma, Shaun Ramroop, Taskeen Khan, Yamile Valdes Gonzalez, Weimar Kunz Sebba Barroso, Frida L Plavnik, Eric Zuniga, Ana María Grassani, Carlos Tajer, Ezequiel Zaidel, Marcos J Marin, Shana Cyr-Philbert, Ignacio Amorin, Miguel Angel Diaz Aguilera, Luiz Bortolotto, Alvaro Avezum, Antonio Luiz P Ribeiro, Sheldon Tobe, Teresa Aumala, Sonia Angell, Pablo Lavados, Sheila Ouriques Martins, Ana Munera Echeverri, Marc G Jaffe, Dorairaj Prabhakaran, Gianfranco Parati, Xin Hua Zhang, Anthony Rodgers, Salim Yusuf, Paul K Whelton, Pedro Ordunez\",\"doi\":\"10.5334/gh.1428\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>HEARTS in the Americas is the regional adaptation of the WHO Global HEARTS Initiative, aimed at helping countries enhance hypertension and cardiovascular disease (CVD) risk management in primary care settings. Its core implementation tool, the HEARTS Clinical Pathway, has been adopted by 28 countries. To improve the care of hypertension, diabetes, and chronic kidney disease (CKD), HEARTS 2.0 was developed as a three-phase process to integrate evidence-based interventions into a unified care pathway, ensuring consistency across fragmented guidelines. This paper focuses on Phase 1, highlighting targeted interventions to improve and update the HEARTS Clinical Pathway.</p><p><strong>Methods: </strong>First, the coordinating group defined the project's scope, objectives, principles, methodological framework, and tools. Second, international experts from different disciplines proposed interventions to enhance the HEARTS Clinical Pathway. Third, the coordinating group harmonized these proposals into unique interventions. Fourth, experts appraised the appropriateness of the proposed interventions on a 1-to-9 scale using the adapted RAND/UCLA Appropriateness Method. Finally, interventions with a median score above 6 were deemed appropriate and selected as candidates to enhance the HEARTS Clinical Pathway.</p><p><strong>Results: </strong>Building on the existing HEARTS Clinical Pathway, 45 unique interventions were selected, including community-based screening, early detection and management of risk factors, lower blood pressure thresholds for diagnosing hypertension in high-CVD-risk patients, reinforcement of single-pill combination therapy, inclusion of sodium-glucose cotransporter-2 inhibitors for patients with diabetes, CKD, or heart failure, expanded roles for non-physician health workers in team-based care, and strengthened clinical documentation, monitoring, and evaluation.</p><p><strong>Conclusion: </strong>HEARTS 2.0 Phase 1 identifies key interventions to integrate and improve hypertension and cardiovascular-kidney-metabolic care within primary care, enabling their seamless incorporation into a unified and effective clinical pathway. This process will inform an update to the HEARTS Clinical Pathway, optimizing resources, reducing care fragmentation, improving care delivery, and advancing health equity, thereby supporting global efforts to combat the leading causes of death and disability.</p>\",\"PeriodicalId\":56018,\"journal\":{\"name\":\"Global Heart\",\"volume\":\"20 1\",\"pages\":\"45\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-05-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12124280/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Global Heart\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5334/gh.1428\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5334/gh.1428","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Candidate Interventions for Integrating Hypertension and Cardiovascular-Kidney-Metabolic Care in Primary Health Settings: HEARTS 2.0 Phase 1.
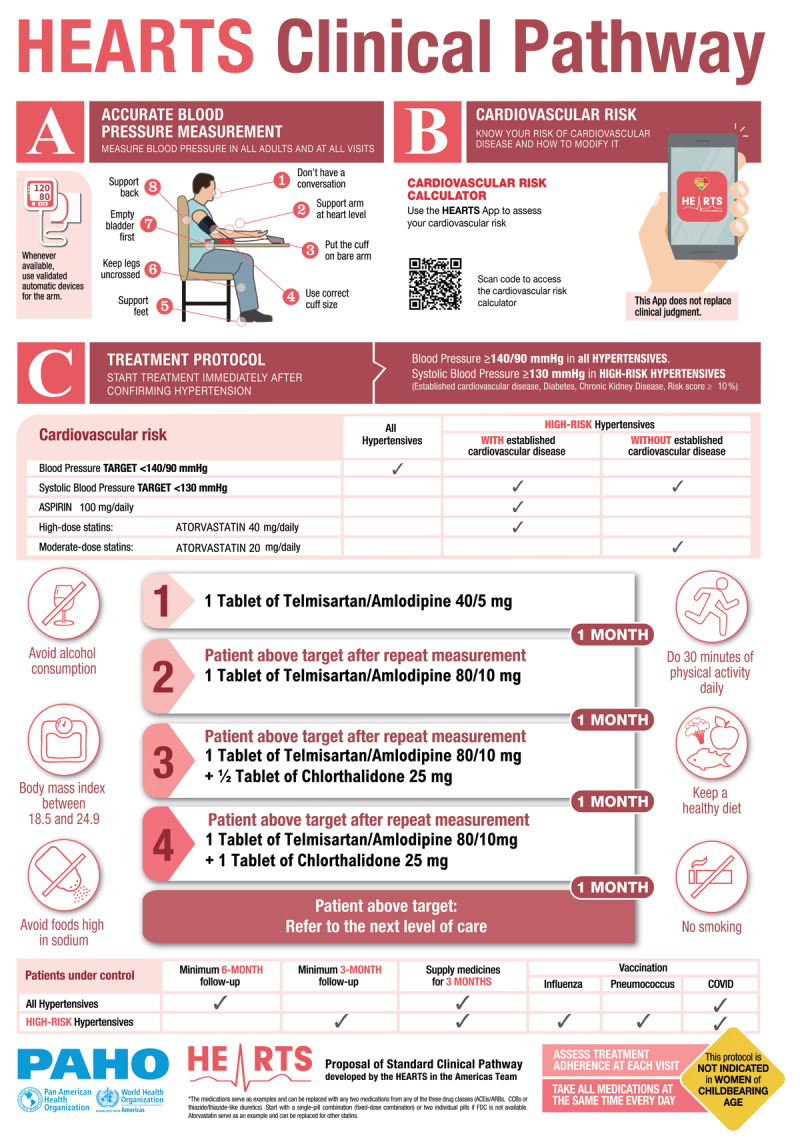
Background: HEARTS in the Americas is the regional adaptation of the WHO Global HEARTS Initiative, aimed at helping countries enhance hypertension and cardiovascular disease (CVD) risk management in primary care settings. Its core implementation tool, the HEARTS Clinical Pathway, has been adopted by 28 countries. To improve the care of hypertension, diabetes, and chronic kidney disease (CKD), HEARTS 2.0 was developed as a three-phase process to integrate evidence-based interventions into a unified care pathway, ensuring consistency across fragmented guidelines. This paper focuses on Phase 1, highlighting targeted interventions to improve and update the HEARTS Clinical Pathway.
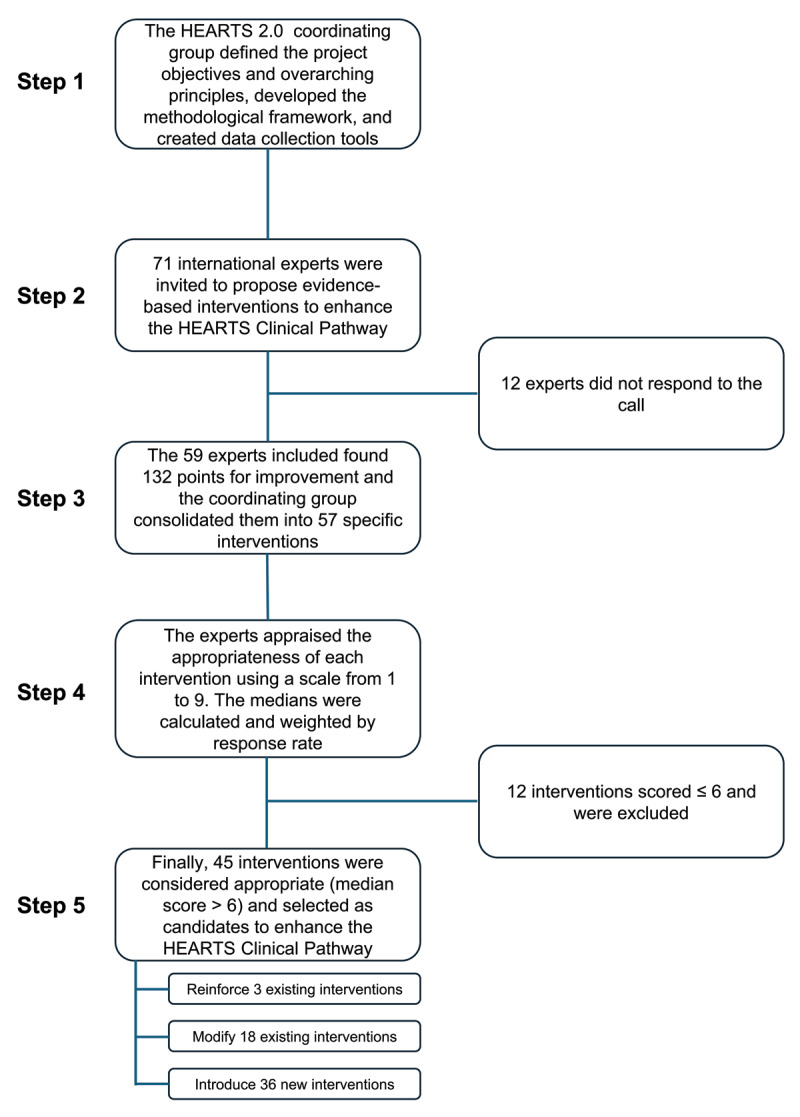
Methods: First, the coordinating group defined the project's scope, objectives, principles, methodological framework, and tools. Second, international experts from different disciplines proposed interventions to enhance the HEARTS Clinical Pathway. Third, the coordinating group harmonized these proposals into unique interventions. Fourth, experts appraised the appropriateness of the proposed interventions on a 1-to-9 scale using the adapted RAND/UCLA Appropriateness Method. Finally, interventions with a median score above 6 were deemed appropriate and selected as candidates to enhance the HEARTS Clinical Pathway.
Results: Building on the existing HEARTS Clinical Pathway, 45 unique interventions were selected, including community-based screening, early detection and management of risk factors, lower blood pressure thresholds for diagnosing hypertension in high-CVD-risk patients, reinforcement of single-pill combination therapy, inclusion of sodium-glucose cotransporter-2 inhibitors for patients with diabetes, CKD, or heart failure, expanded roles for non-physician health workers in team-based care, and strengthened clinical documentation, monitoring, and evaluation.
Conclusion: HEARTS 2.0 Phase 1 identifies key interventions to integrate and improve hypertension and cardiovascular-kidney-metabolic care within primary care, enabling their seamless incorporation into a unified and effective clinical pathway. This process will inform an update to the HEARTS Clinical Pathway, optimizing resources, reducing care fragmentation, improving care delivery, and advancing health equity, thereby supporting global efforts to combat the leading causes of death and disability.
Global HeartMedicine-Cardiology and Cardiovascular Medicine
CiteScore
5.70
自引率
5.40%
发文量
77
审稿时长
5 weeks
期刊介绍:
Global Heart offers a forum for dialogue and education on research, developments, trends, solutions and public health programs related to the prevention and control of cardiovascular diseases (CVDs) worldwide, with a special focus on low- and middle-income countries (LMICs). Manuscripts should address not only the extent or epidemiology of the problem, but also describe interventions to effectively control and prevent CVDs and the underlying factors. The emphasis should be on approaches applicable in settings with limited resources.
Economic evaluations of successful interventions are particularly welcome. We will also consider negative findings if important. While reports of hospital or clinic-based treatments are not excluded, particularly if they have broad implications for cost-effective disease control or prevention, we give priority to papers addressing community-based activities. We encourage submissions on cardiovascular surveillance and health policies, professional education, ethical issues and technological innovations related to prevention.
Global Heart is particularly interested in publishing data from updated national or regional demographic health surveys, World Health Organization or Global Burden of Disease data, large clinical disease databases or registries. Systematic reviews or meta-analyses on globally relevant topics are welcome. We will also consider clinical research that has special relevance to LMICs, e.g. using validated instruments to assess health-related quality-of-life in patients from LMICs, innovative diagnostic-therapeutic applications, real-world effectiveness clinical trials, research methods (innovative methodologic papers, with emphasis on low-cost research methods or novel application of methods in low resource settings), and papers pertaining to cardiovascular health promotion and policy (quantitative evaluation of health programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


