Rezan Ashayeri Ahmadabad, Mohammed Almekhlafi, P N Sylaja, Aviraj Deshmukh, Jesse Dawson, Aleksandra Pikula, Muhammad Shazam Hussain, Yiran Zhang, Negar Asdaghi, Sung-Ii Sohn, Mohammad Wasay, Ashfaq Shuaib, Brian Buck, Mahesh Pundlik Kate
{"title":"急性卒中再灌注治疗患者复发性卒中预防策略(copprime研究调查)。","authors":"Rezan Ashayeri Ahmadabad, Mohammed Almekhlafi, P N Sylaja, Aviraj Deshmukh, Jesse Dawson, Aleksandra Pikula, Muhammad Shazam Hussain, Yiran Zhang, Negar Asdaghi, Sung-Ii Sohn, Mohammad Wasay, Ashfaq Shuaib, Brian Buck, Mahesh Pundlik Kate","doi":"10.1159/000546654","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients who have undergone reperfusion treatments, like all ischemic stroke patients, are at risk of recurrent ischemic strokes in the first 90 days. Current guidelines recommend single antiplatelet therapy for secondary prevention at variable time points after the procedure. This study assessed the practices and perspectives of healthcare professionals on the use of dual antiplatelet therapy in patients with non-cardioembolic ischemic stroke who have undergone reperfusion therapy.</p><p><strong>Methods: </strong>We conducted a multinational cross-sectional web-based survey using Qualtrics involving neurologists and non-neurologist stroke physicians (including neurosurgeons, interventional neuroradiologists, and internal medicine physicians). Participants were asked about their current practices and presented with six structured case scenarios to determine their treatment preferences. In the case scenarios, we assessed their willingness to randomize to a clinical trial comparing single versus dual antiplatelets. Multinomial logistic regression analysis was performed to assess the relationship between demographic characteristics and willingness to randomize.</p><p><strong>Results: </strong>A total of 278 clinicians from 26 countries participated in the survey. The most common continent of practice was Asia (155/278; 55.9%). The most common area of practice was neurology (220/278; 79.1%), with most participants having 5-15 years of experience (115/278; 41.5%) and working in comprehensive stroke centers (205/278; 73.9%). Antiplatelet Choice: For a small infarct post-intravenous thrombolysis and endovascular thrombectomy (EVT), 194/278 (69.8%) preferred aspirin, and 49/278 (17.6%) chose a dual antiplatelet strategy with aspirin and clopidogrel. Loading of Antiplatelet: A total of 121/278 (43.5%) indicated they would not administer a loading dose in cases even with small final infarctions. Timing of Antiplatelet Initiation: Preferences varied; 61/278 (21.7%) considered early initiation immediately post-EVT, and 103/278 (37.2%) considered 24 h post-EVT. Willingness to Randomize: A total of 16/278 (77.7%) were willing or would consider randomizing in a clinical trial with dual antiplatelet. On regression analyses, the willingness to randomize was influenced by years of practice and the local volume of reperfusion therapy.</p><p><strong>Conclusion: </strong>Antiplatelet management for secondary stroke prevention in patients with non-cardioembolic ischemic stroke following reperfusion therapy is variable. However, more than three-fourths of participants were willing to consider randomization to a clinical trial exploring the prevention of recurrent stroke after reperfusion therapy.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":" ","pages":"162-172"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237293/pdf/","citationCount":"0","resultStr":"{\"title\":\"Recurrent Stroke Prevention Strategies in Patients Receiving Acute Stroke Reperfusion Therapies (CoPrime Study Survey).\",\"authors\":\"Rezan Ashayeri Ahmadabad, Mohammed Almekhlafi, P N Sylaja, Aviraj Deshmukh, Jesse Dawson, Aleksandra Pikula, Muhammad Shazam Hussain, Yiran Zhang, Negar Asdaghi, Sung-Ii Sohn, Mohammad Wasay, Ashfaq Shuaib, Brian Buck, Mahesh Pundlik Kate\",\"doi\":\"10.1159/000546654\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Patients who have undergone reperfusion treatments, like all ischemic stroke patients, are at risk of recurrent ischemic strokes in the first 90 days. Current guidelines recommend single antiplatelet therapy for secondary prevention at variable time points after the procedure. This study assessed the practices and perspectives of healthcare professionals on the use of dual antiplatelet therapy in patients with non-cardioembolic ischemic stroke who have undergone reperfusion therapy.</p><p><strong>Methods: </strong>We conducted a multinational cross-sectional web-based survey using Qualtrics involving neurologists and non-neurologist stroke physicians (including neurosurgeons, interventional neuroradiologists, and internal medicine physicians). Participants were asked about their current practices and presented with six structured case scenarios to determine their treatment preferences. In the case scenarios, we assessed their willingness to randomize to a clinical trial comparing single versus dual antiplatelets. Multinomial logistic regression analysis was performed to assess the relationship between demographic characteristics and willingness to randomize.</p><p><strong>Results: </strong>A total of 278 clinicians from 26 countries participated in the survey. The most common continent of practice was Asia (155/278; 55.9%). The most common area of practice was neurology (220/278; 79.1%), with most participants having 5-15 years of experience (115/278; 41.5%) and working in comprehensive stroke centers (205/278; 73.9%). Antiplatelet Choice: For a small infarct post-intravenous thrombolysis and endovascular thrombectomy (EVT), 194/278 (69.8%) preferred aspirin, and 49/278 (17.6%) chose a dual antiplatelet strategy with aspirin and clopidogrel. Loading of Antiplatelet: A total of 121/278 (43.5%) indicated they would not administer a loading dose in cases even with small final infarctions. Timing of Antiplatelet Initiation: Preferences varied; 61/278 (21.7%) considered early initiation immediately post-EVT, and 103/278 (37.2%) considered 24 h post-EVT. Willingness to Randomize: A total of 16/278 (77.7%) were willing or would consider randomizing in a clinical trial with dual antiplatelet. On regression analyses, the willingness to randomize was influenced by years of practice and the local volume of reperfusion therapy.</p><p><strong>Conclusion: </strong>Antiplatelet management for secondary stroke prevention in patients with non-cardioembolic ischemic stroke following reperfusion therapy is variable. However, more than three-fourths of participants were willing to consider randomization to a clinical trial exploring the prevention of recurrent stroke after reperfusion therapy.</p>\",\"PeriodicalId\":45709,\"journal\":{\"name\":\"Cerebrovascular Diseases Extra\",\"volume\":\" \",\"pages\":\"162-172\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237293/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cerebrovascular Diseases Extra\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000546654\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000546654","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Recurrent Stroke Prevention Strategies in Patients Receiving Acute Stroke Reperfusion Therapies (CoPrime Study Survey).
Introduction: Patients who have undergone reperfusion treatments, like all ischemic stroke patients, are at risk of recurrent ischemic strokes in the first 90 days. Current guidelines recommend single antiplatelet therapy for secondary prevention at variable time points after the procedure. This study assessed the practices and perspectives of healthcare professionals on the use of dual antiplatelet therapy in patients with non-cardioembolic ischemic stroke who have undergone reperfusion therapy.
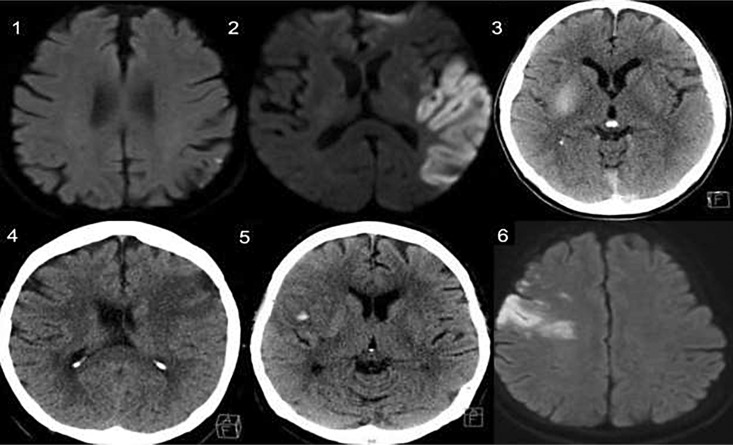
Methods: We conducted a multinational cross-sectional web-based survey using Qualtrics involving neurologists and non-neurologist stroke physicians (including neurosurgeons, interventional neuroradiologists, and internal medicine physicians). Participants were asked about their current practices and presented with six structured case scenarios to determine their treatment preferences. In the case scenarios, we assessed their willingness to randomize to a clinical trial comparing single versus dual antiplatelets. Multinomial logistic regression analysis was performed to assess the relationship between demographic characteristics and willingness to randomize.
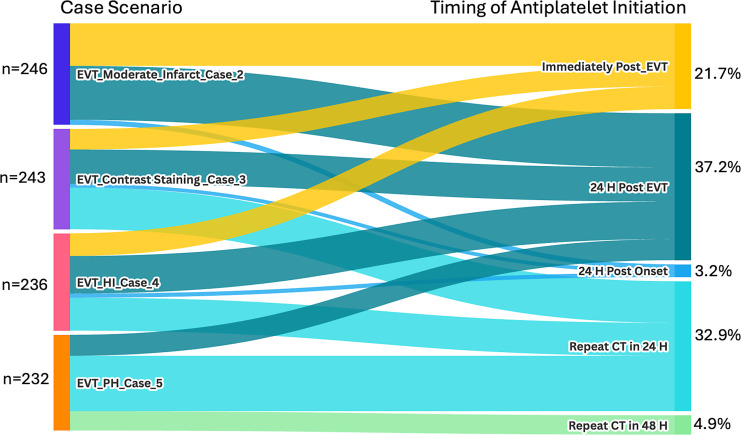
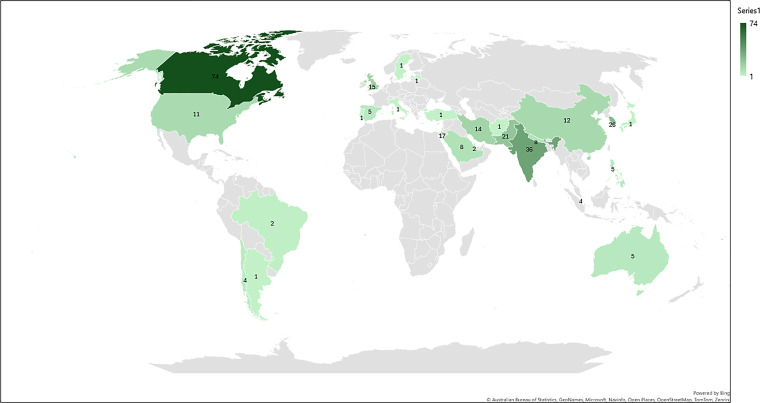
Results: A total of 278 clinicians from 26 countries participated in the survey. The most common continent of practice was Asia (155/278; 55.9%). The most common area of practice was neurology (220/278; 79.1%), with most participants having 5-15 years of experience (115/278; 41.5%) and working in comprehensive stroke centers (205/278; 73.9%). Antiplatelet Choice: For a small infarct post-intravenous thrombolysis and endovascular thrombectomy (EVT), 194/278 (69.8%) preferred aspirin, and 49/278 (17.6%) chose a dual antiplatelet strategy with aspirin and clopidogrel. Loading of Antiplatelet: A total of 121/278 (43.5%) indicated they would not administer a loading dose in cases even with small final infarctions. Timing of Antiplatelet Initiation: Preferences varied; 61/278 (21.7%) considered early initiation immediately post-EVT, and 103/278 (37.2%) considered 24 h post-EVT. Willingness to Randomize: A total of 16/278 (77.7%) were willing or would consider randomizing in a clinical trial with dual antiplatelet. On regression analyses, the willingness to randomize was influenced by years of practice and the local volume of reperfusion therapy.
Conclusion: Antiplatelet management for secondary stroke prevention in patients with non-cardioembolic ischemic stroke following reperfusion therapy is variable. However, more than three-fourths of participants were willing to consider randomization to a clinical trial exploring the prevention of recurrent stroke after reperfusion therapy.
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


