John D Fisher, Thomas Aldrich, Linda Lewallen, Jason Adkins, Mohammad H Mustehsan, Yvette Ash, Marjan Rahmanian, Suzanne Knowlton, Vanessa Taylor, Marianne O'Shea, Vilma Joseph
{"title":"已知或有阻塞性睡眠呼吸暂停(OSA)危险因素的高危患者在心脏电生理(EP)过程中非麻醉医师正压通气和镇静/镇痛的安全性","authors":"John D Fisher, Thomas Aldrich, Linda Lewallen, Jason Adkins, Mohammad H Mustehsan, Yvette Ash, Marjan Rahmanian, Suzanne Knowlton, Vanessa Taylor, Marianne O'Shea, Vilma Joseph","doi":"10.1007/s10840-025-02044-5","DOIUrl":null,"url":null,"abstract":"<p><p>Concerns exist about the safety of non-anesthesiologist positive pressure ventilation with sedation/analgesia during cardiac electrophysiology (EP) procedures in high-risk patients with known or risk factors such as obstructive sleep apnea (OSA). This is magnified if the procedures are done outside of intensive care areas or outside of hospital policies and procedures rules.</p><p><strong>Background: </strong>Noninvasive positive pressure ventilation mask ventilation (NIPPV including continuous or bilevel positive airway pressure-CPAP/BiPAP) with sedation/analgesia is typically limited to hospital units staffed by pulmonary-intensive care or anesthesiology personnel, with monitoring by respiratory therapists or specifically trained nursing staff. NIPPV with sedation has raised concerns if delivered by laboratory staff in procedure rooms, especially in high-risk patients. Literature is sparse on this topic. NIPPV as described is routine at some institutions and prohibited at others. We aimed (1) to test the safety and efficacy of NIPPV with sedation prescribed by cardiologists and administered by trained nurses in a prospective cohort of high-risk patients and (2) to provide data that, if favorable, could lead to revisions of institutional policies.</p><p><strong>Methods: </strong>We enrolled 50 consecutive consenting patients with known or at high risk for OSA. Three were then excluded (did not qualify, or procedure canceled). Procedures in 47 patients included 21 ICD implants (12 with defibrillation testing), 8 pacemaker implants, 11 ablations, and 7 cardioversions; some patients had combined procedures, e.g., \"ablate & pace.\" Standard NIPPV settings were used. Staff were trained in general NIPPV device monitoring and management. Data collected included vital signs, O<sub>2</sub> saturations, hypercapnia, demographics, toleration of NIPPV, and complications.</p><p><strong>Results: </strong>There were no NIPPV-related complications and no long-term adverse sequelae in the 47 patients who participated in the protocol. No patient required intubation or urgent rescue from an anesthesiologist. Most patients (45) tolerated NIPPV including patients without prior experience.</p><p><strong>Conclusions: </strong>NIPPV with sedation can be safely delivered in high-risk OSA patients by trained non-anesthesiologist/pulmonary/intensive care personnel in an EP lab setting. Policy and procedure manuals may benefit from revision.</p>","PeriodicalId":520675,"journal":{"name":"Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing","volume":" ","pages":"1327-1337"},"PeriodicalIF":2.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399687/pdf/","citationCount":"0","resultStr":"{\"title\":\"Safety of non-anesthesiologist positive pressure ventilation and sedation/analgesia during cardiac electrophysiology (EP) procedures in high-risk patients with known or risk factors for obstructive sleep apnea (OSA).\",\"authors\":\"John D Fisher, Thomas Aldrich, Linda Lewallen, Jason Adkins, Mohammad H Mustehsan, Yvette Ash, Marjan Rahmanian, Suzanne Knowlton, Vanessa Taylor, Marianne O'Shea, Vilma Joseph\",\"doi\":\"10.1007/s10840-025-02044-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Concerns exist about the safety of non-anesthesiologist positive pressure ventilation with sedation/analgesia during cardiac electrophysiology (EP) procedures in high-risk patients with known or risk factors such as obstructive sleep apnea (OSA). This is magnified if the procedures are done outside of intensive care areas or outside of hospital policies and procedures rules.</p><p><strong>Background: </strong>Noninvasive positive pressure ventilation mask ventilation (NIPPV including continuous or bilevel positive airway pressure-CPAP/BiPAP) with sedation/analgesia is typically limited to hospital units staffed by pulmonary-intensive care or anesthesiology personnel, with monitoring by respiratory therapists or specifically trained nursing staff. NIPPV with sedation has raised concerns if delivered by laboratory staff in procedure rooms, especially in high-risk patients. Literature is sparse on this topic. NIPPV as described is routine at some institutions and prohibited at others. We aimed (1) to test the safety and efficacy of NIPPV with sedation prescribed by cardiologists and administered by trained nurses in a prospective cohort of high-risk patients and (2) to provide data that, if favorable, could lead to revisions of institutional policies.</p><p><strong>Methods: </strong>We enrolled 50 consecutive consenting patients with known or at high risk for OSA. Three were then excluded (did not qualify, or procedure canceled). Procedures in 47 patients included 21 ICD implants (12 with defibrillation testing), 8 pacemaker implants, 11 ablations, and 7 cardioversions; some patients had combined procedures, e.g., \\\"ablate & pace.\\\" Standard NIPPV settings were used. Staff were trained in general NIPPV device monitoring and management. Data collected included vital signs, O<sub>2</sub> saturations, hypercapnia, demographics, toleration of NIPPV, and complications.</p><p><strong>Results: </strong>There were no NIPPV-related complications and no long-term adverse sequelae in the 47 patients who participated in the protocol. No patient required intubation or urgent rescue from an anesthesiologist. Most patients (45) tolerated NIPPV including patients without prior experience.</p><p><strong>Conclusions: </strong>NIPPV with sedation can be safely delivered in high-risk OSA patients by trained non-anesthesiologist/pulmonary/intensive care personnel in an EP lab setting. Policy and procedure manuals may benefit from revision.</p>\",\"PeriodicalId\":520675,\"journal\":{\"name\":\"Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing\",\"volume\":\" \",\"pages\":\"1327-1337\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12399687/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s10840-025-02044-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s10840-025-02044-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Safety of non-anesthesiologist positive pressure ventilation and sedation/analgesia during cardiac electrophysiology (EP) procedures in high-risk patients with known or risk factors for obstructive sleep apnea (OSA).
Concerns exist about the safety of non-anesthesiologist positive pressure ventilation with sedation/analgesia during cardiac electrophysiology (EP) procedures in high-risk patients with known or risk factors such as obstructive sleep apnea (OSA). This is magnified if the procedures are done outside of intensive care areas or outside of hospital policies and procedures rules.
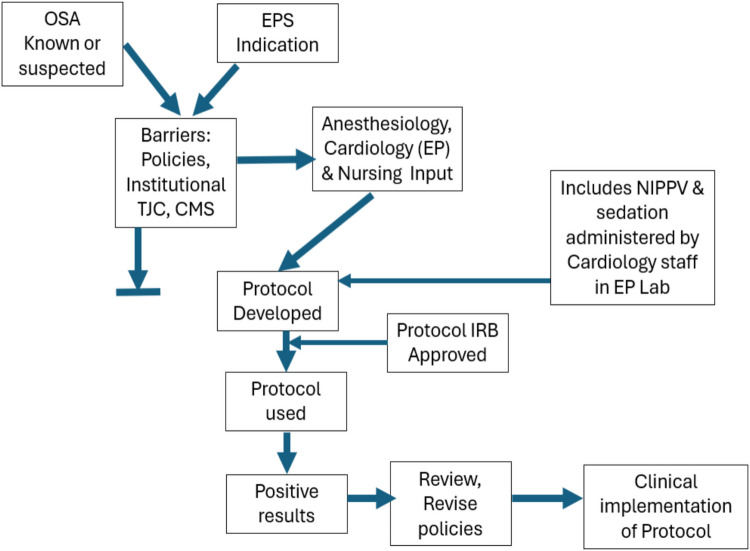
Background: Noninvasive positive pressure ventilation mask ventilation (NIPPV including continuous or bilevel positive airway pressure-CPAP/BiPAP) with sedation/analgesia is typically limited to hospital units staffed by pulmonary-intensive care or anesthesiology personnel, with monitoring by respiratory therapists or specifically trained nursing staff. NIPPV with sedation has raised concerns if delivered by laboratory staff in procedure rooms, especially in high-risk patients. Literature is sparse on this topic. NIPPV as described is routine at some institutions and prohibited at others. We aimed (1) to test the safety and efficacy of NIPPV with sedation prescribed by cardiologists and administered by trained nurses in a prospective cohort of high-risk patients and (2) to provide data that, if favorable, could lead to revisions of institutional policies.
Methods: We enrolled 50 consecutive consenting patients with known or at high risk for OSA. Three were then excluded (did not qualify, or procedure canceled). Procedures in 47 patients included 21 ICD implants (12 with defibrillation testing), 8 pacemaker implants, 11 ablations, and 7 cardioversions; some patients had combined procedures, e.g., "ablate & pace." Standard NIPPV settings were used. Staff were trained in general NIPPV device monitoring and management. Data collected included vital signs, O2 saturations, hypercapnia, demographics, toleration of NIPPV, and complications.
Results: There were no NIPPV-related complications and no long-term adverse sequelae in the 47 patients who participated in the protocol. No patient required intubation or urgent rescue from an anesthesiologist. Most patients (45) tolerated NIPPV including patients without prior experience.
Conclusions: NIPPV with sedation can be safely delivered in high-risk OSA patients by trained non-anesthesiologist/pulmonary/intensive care personnel in an EP lab setting. Policy and procedure manuals may benefit from revision.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


