Alessio Finocchiaro, Anna Tylecki, Silvia Viganò, Alessandro Bertini, Vincenzo Ficarra, Ettore Di Trapani, Andrea Salonia, Alberto Briganti, Francesco Montorsi, Giovanni Lughezzani, Nicolò Buffi, Akshay Sood, Craig Rogers, Firas Abdollah
{"title":"社会经济差异与膀胱癌诊断阶段:一项全州范围的队列分析。","authors":"Alessio Finocchiaro, Anna Tylecki, Silvia Viganò, Alessandro Bertini, Vincenzo Ficarra, Ettore Di Trapani, Andrea Salonia, Alberto Briganti, Francesco Montorsi, Giovanni Lughezzani, Nicolò Buffi, Akshay Sood, Craig Rogers, Firas Abdollah","doi":"10.1093/jncics/pkaf054","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bladder cancer is the ninth most common cancer worldwide. Despite its prevalence, large-scale studies on the relationship between socioeconomic disparities and disease stage at presentation are lacking. This study examines the association between the Area Deprivation Index (ADI), a robust measure of socioeconomic status, and stage at diagnosis among bladder cancer patients.</p><p><strong>Methods: </strong>Patients diagnosed with bladder cancer (any TNM stage) from the Michigan Department of Health and Human Services (2004-2019) were retrospectively analyzed. ADI was assigned based on patients' residential census-block group and stratified into quartiles, with the fourth quartile (ADI 75-100) representing the most deprived. Multivariable logistic regression tested the impact of ADI on advanced disease stages (muscle invasive disease [≥T2], positive nodal status [cN+], metastatic disease [cM+]).</p><p><strong>Results: </strong>Among 29 010 patients, the majority were non-Hispanic White (92%), males (75%), and residents in metropolitan areas (81%). Patients in the third and fourth ADI quartiles had higher rates of ≥T2 (22%, 24.5%) compared with the first and second quartiles (18%, 19.5%) (P < .001), as well as increased rates of cN+ (3.4%, 3.7%) and cM+ (2.8%, 3.2%) (P < .001). Multivariable regression showed that each 10-unit rise in ADI increased odds of T2 by 4% (95% CI = 1.03 to 1.06, P < .001), cN+ by 4% (95% CI = 1.01 to 1.07, P = .038), and cM+ by 6% (95% CI = 1.02 to 1.09, P = .003).</p><p><strong>Conclusion: </strong>Higher ADI correlates with advanced bladder cancer stages at diagnosis. Addressing these disparities is essential to improve outcomes in bladder cancer care.</p>","PeriodicalId":14681,"journal":{"name":"JNCI Cancer Spectrum","volume":" ","pages":""},"PeriodicalIF":4.1000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12274062/pdf/","citationCount":"0","resultStr":"{\"title\":\"Socioeconomic disparities and bladder cancer stage at diagnosis: a statewide cohort analysis.\",\"authors\":\"Alessio Finocchiaro, Anna Tylecki, Silvia Viganò, Alessandro Bertini, Vincenzo Ficarra, Ettore Di Trapani, Andrea Salonia, Alberto Briganti, Francesco Montorsi, Giovanni Lughezzani, Nicolò Buffi, Akshay Sood, Craig Rogers, Firas Abdollah\",\"doi\":\"10.1093/jncics/pkaf054\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Bladder cancer is the ninth most common cancer worldwide. Despite its prevalence, large-scale studies on the relationship between socioeconomic disparities and disease stage at presentation are lacking. This study examines the association between the Area Deprivation Index (ADI), a robust measure of socioeconomic status, and stage at diagnosis among bladder cancer patients.</p><p><strong>Methods: </strong>Patients diagnosed with bladder cancer (any TNM stage) from the Michigan Department of Health and Human Services (2004-2019) were retrospectively analyzed. ADI was assigned based on patients' residential census-block group and stratified into quartiles, with the fourth quartile (ADI 75-100) representing the most deprived. Multivariable logistic regression tested the impact of ADI on advanced disease stages (muscle invasive disease [≥T2], positive nodal status [cN+], metastatic disease [cM+]).</p><p><strong>Results: </strong>Among 29 010 patients, the majority were non-Hispanic White (92%), males (75%), and residents in metropolitan areas (81%). Patients in the third and fourth ADI quartiles had higher rates of ≥T2 (22%, 24.5%) compared with the first and second quartiles (18%, 19.5%) (P < .001), as well as increased rates of cN+ (3.4%, 3.7%) and cM+ (2.8%, 3.2%) (P < .001). Multivariable regression showed that each 10-unit rise in ADI increased odds of T2 by 4% (95% CI = 1.03 to 1.06, P < .001), cN+ by 4% (95% CI = 1.01 to 1.07, P = .038), and cM+ by 6% (95% CI = 1.02 to 1.09, P = .003).</p><p><strong>Conclusion: </strong>Higher ADI correlates with advanced bladder cancer stages at diagnosis. Addressing these disparities is essential to improve outcomes in bladder cancer care.</p>\",\"PeriodicalId\":14681,\"journal\":{\"name\":\"JNCI Cancer Spectrum\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12274062/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JNCI Cancer Spectrum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jncics/pkaf054\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JNCI Cancer Spectrum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jncics/pkaf054","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Socioeconomic disparities and bladder cancer stage at diagnosis: a statewide cohort analysis.
Background: Bladder cancer is the ninth most common cancer worldwide. Despite its prevalence, large-scale studies on the relationship between socioeconomic disparities and disease stage at presentation are lacking. This study examines the association between the Area Deprivation Index (ADI), a robust measure of socioeconomic status, and stage at diagnosis among bladder cancer patients.
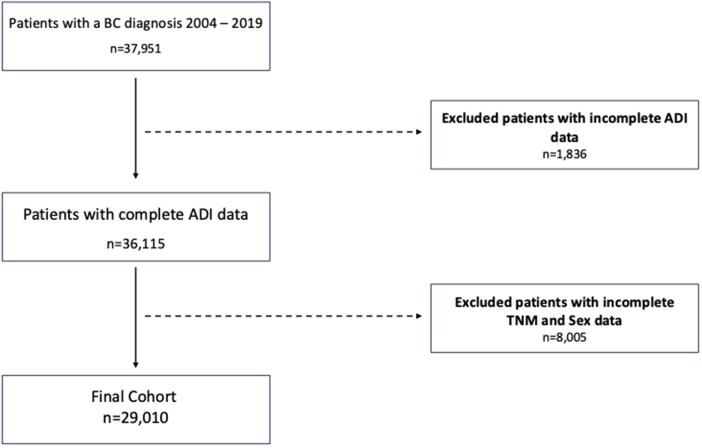
Methods: Patients diagnosed with bladder cancer (any TNM stage) from the Michigan Department of Health and Human Services (2004-2019) were retrospectively analyzed. ADI was assigned based on patients' residential census-block group and stratified into quartiles, with the fourth quartile (ADI 75-100) representing the most deprived. Multivariable logistic regression tested the impact of ADI on advanced disease stages (muscle invasive disease [≥T2], positive nodal status [cN+], metastatic disease [cM+]).
Results: Among 29 010 patients, the majority were non-Hispanic White (92%), males (75%), and residents in metropolitan areas (81%). Patients in the third and fourth ADI quartiles had higher rates of ≥T2 (22%, 24.5%) compared with the first and second quartiles (18%, 19.5%) (P < .001), as well as increased rates of cN+ (3.4%, 3.7%) and cM+ (2.8%, 3.2%) (P < .001). Multivariable regression showed that each 10-unit rise in ADI increased odds of T2 by 4% (95% CI = 1.03 to 1.06, P < .001), cN+ by 4% (95% CI = 1.01 to 1.07, P = .038), and cM+ by 6% (95% CI = 1.02 to 1.09, P = .003).
Conclusion: Higher ADI correlates with advanced bladder cancer stages at diagnosis. Addressing these disparities is essential to improve outcomes in bladder cancer care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


