Yub Raj Sedhai, Priyanka Bhat, Roshan Acharya, Nada Qaiser Qureshi, Fawaz Mohammed, Irfan Waheed, Tahir Muhammad Abdullah Khan, Muhammad Altaf Ahmed, Nisarfathima Kazimuddin, Akinchan Kafle, Rodney T Steff, Karan Singh
{"title":"胸膜内组织纤溶酶原激活剂和脱氧核糖核酸酶在复杂胸腔积液和脓胸中的作用,临床结果和预测因素。","authors":"Yub Raj Sedhai, Priyanka Bhat, Roshan Acharya, Nada Qaiser Qureshi, Fawaz Mohammed, Irfan Waheed, Tahir Muhammad Abdullah Khan, Muhammad Altaf Ahmed, Nisarfathima Kazimuddin, Akinchan Kafle, Rodney T Steff, Karan Singh","doi":"10.1177/17534666251343711","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Complex pleural effusion and empyema (CPPE) is treated with intrapleural fibrinolytic therapy (IPFT) using tissue plasminogen activator (tPA) and deoxyribonuclease (DNase) We present our single-center retrospective observational data using a simplified regimen of coadministering six divided doses of tPA and DNase over the course of 3 days.</p><p><strong>Objective: </strong>To study the safety, utility, and clinical outcomes of IPFT.</p><p><strong>Design: </strong>This is a single-center retrospective study of patients who received co-administration tPA/DNase for CPPE over a period of 5 years. The primary outcome was successful treatment without the need for surgery. Secondary outcomes were bleeding risk, post-procedural pain, treatment complications, and all-cause mortality at 30 days and 6 months. We have tested the clinical role RAPID score (Renal function measured as urea, Age, fluid Purulence, Infection source, Dietary status measured as albumin) to predict treatment success, and all-cause mortality at 6 months.</p><p><strong>Results: </strong>A total of (<i>n</i> = 55) patients were included in the study. The mean age of the population studied was 67 (Interquartile range 57-74), including 47.3% male and 52.7% Female. 92.7% of the population studied was Caucasian. Comorbidities including chronic obstructive pulmonary disease, congestive heart failure, and Diabetes mellitus were present in 41.8%, 41.8%, and 43.6.% respectively. Patients were treated with tube thoracostomy with 14 French percutaneous pigtail catheters in 47 (85.5%) or 28-32 French chest tubes in 8 (14.5%) patients. Twenty-nine percent (16) of patients had acceptable clinical and radiographic improvement and did not require additional surgical or radiological intervention. Seventy-one percent (39) of patients required additional surgical drainage; video-assisted thoracoscopic surgery in 37, and open thoracotomy in 2 patients. The discriminating ability of the RAPID score for treatment success after IPFT was found to be poor (AUC: 0.601, 95% CI: 0.429-0.773, <i>p</i> = 0.24). All-cause mortality at 6 months was 23.6% (13) of patients. The predictive ability of the RAPID score for mortality at 6 months was found to be poor (AUC: 0.640, 95% CI: 0.478-0.802, <i>p</i> = 0.13). The optimal cutoff for the RAPID score for mortality was ⩾4, with 84.6% sensitivity and 46.3% specificity.</p><p><strong>Conclusion: </strong>Results of our single-center study suggest that IPFT can be safely adopted by small and mid-sized clinical centers, as the risk of bleeding is low. The results of coadministering tPA and DNase are safe, and it reduces the need for surgical intervention in nearly one-third of patients.</p>","PeriodicalId":22884,"journal":{"name":"Therapeutic Advances in Respiratory Disease","volume":"19 ","pages":"17534666251343711"},"PeriodicalIF":3.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12126679/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intrapleural tissue plasminogen activator and deoxyribonuclease in complex pleural effusion and empyema, clinical outcomes, and predictors.\",\"authors\":\"Yub Raj Sedhai, Priyanka Bhat, Roshan Acharya, Nada Qaiser Qureshi, Fawaz Mohammed, Irfan Waheed, Tahir Muhammad Abdullah Khan, Muhammad Altaf Ahmed, Nisarfathima Kazimuddin, Akinchan Kafle, Rodney T Steff, Karan Singh\",\"doi\":\"10.1177/17534666251343711\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Complex pleural effusion and empyema (CPPE) is treated with intrapleural fibrinolytic therapy (IPFT) using tissue plasminogen activator (tPA) and deoxyribonuclease (DNase) We present our single-center retrospective observational data using a simplified regimen of coadministering six divided doses of tPA and DNase over the course of 3 days.</p><p><strong>Objective: </strong>To study the safety, utility, and clinical outcomes of IPFT.</p><p><strong>Design: </strong>This is a single-center retrospective study of patients who received co-administration tPA/DNase for CPPE over a period of 5 years. The primary outcome was successful treatment without the need for surgery. Secondary outcomes were bleeding risk, post-procedural pain, treatment complications, and all-cause mortality at 30 days and 6 months. We have tested the clinical role RAPID score (Renal function measured as urea, Age, fluid Purulence, Infection source, Dietary status measured as albumin) to predict treatment success, and all-cause mortality at 6 months.</p><p><strong>Results: </strong>A total of (<i>n</i> = 55) patients were included in the study. The mean age of the population studied was 67 (Interquartile range 57-74), including 47.3% male and 52.7% Female. 92.7% of the population studied was Caucasian. Comorbidities including chronic obstructive pulmonary disease, congestive heart failure, and Diabetes mellitus were present in 41.8%, 41.8%, and 43.6.% respectively. Patients were treated with tube thoracostomy with 14 French percutaneous pigtail catheters in 47 (85.5%) or 28-32 French chest tubes in 8 (14.5%) patients. Twenty-nine percent (16) of patients had acceptable clinical and radiographic improvement and did not require additional surgical or radiological intervention. Seventy-one percent (39) of patients required additional surgical drainage; video-assisted thoracoscopic surgery in 37, and open thoracotomy in 2 patients. The discriminating ability of the RAPID score for treatment success after IPFT was found to be poor (AUC: 0.601, 95% CI: 0.429-0.773, <i>p</i> = 0.24). All-cause mortality at 6 months was 23.6% (13) of patients. The predictive ability of the RAPID score for mortality at 6 months was found to be poor (AUC: 0.640, 95% CI: 0.478-0.802, <i>p</i> = 0.13). The optimal cutoff for the RAPID score for mortality was ⩾4, with 84.6% sensitivity and 46.3% specificity.</p><p><strong>Conclusion: </strong>Results of our single-center study suggest that IPFT can be safely adopted by small and mid-sized clinical centers, as the risk of bleeding is low. The results of coadministering tPA and DNase are safe, and it reduces the need for surgical intervention in nearly one-third of patients.</p>\",\"PeriodicalId\":22884,\"journal\":{\"name\":\"Therapeutic Advances in Respiratory Disease\",\"volume\":\"19 \",\"pages\":\"17534666251343711\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12126679/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Respiratory Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17534666251343711\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17534666251343711","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
背景:使用组织型纤溶酶原激活剂(tPA)和脱氧核糖核酸酶(DNase)进行胸膜内纤溶治疗(IPFT)治疗复杂胸腔积液和脓胸(CPPE)。我们采用简化方案,在3天内共给药6次tPA和DNase,提出了单中心回顾性观察数据。目的:探讨IPFT的安全性、实用性及临床效果。设计:这是一项单中心回顾性研究,研究对象是在5年的时间里接受tPA/DNase联合治疗CPPE的患者。主要结果是治疗成功,无需手术。次要结局是出血风险、术后疼痛、治疗并发症和30天和6个月的全因死亡率。我们已经测试了RAPID评分(以尿素测定肾功能、年龄、液体化脓、感染源、以白蛋白测定饮食状况)在预测治疗成功和6个月全因死亡率方面的临床作用。结果:共纳入(n = 55)例患者。研究人群的平均年龄为67岁(四分位间距为57 ~ 74岁),其中男性占47.3%,女性占52.7%,白种人占92.7%。合并疾病包括慢性阻塞性肺疾病、充血性心力衰竭和糖尿病,分别占41.8%、41.8%和43.6%。分别为%。47例(85.5%)患者行管式开胸术,其中14根经皮法式猪尾导管,8例(14.5%)患者行28-32根法式胸管。29%(16)的患者有可接受的临床和放射学改善,不需要额外的手术或放射干预。71%(39)的患者需要额外的手术引流;视频胸腔镜手术37例,开胸手术2例。发现RAPID评分对IPFT后治疗成功的判别能力较差(AUC: 0.601, 95% CI: 0.429-0.773, p = 0.24)。6个月全因死亡率为23.6%(13例)。RAPID评分对6个月死亡率的预测能力较差(AUC: 0.640, 95% CI: 0.478-0.802, p = 0.13)。死亡率的RAPID评分的最佳截止时间是大于或等于4,具有84.6%的敏感性和46.3%的特异性。结论:我们的单中心研究结果表明,由于出血风险低,IPFT在中小型临床中心可以安全采用。联合使用tPA和DNase的结果是安全的,并且减少了近三分之一患者的手术干预需求。
Intrapleural tissue plasminogen activator and deoxyribonuclease in complex pleural effusion and empyema, clinical outcomes, and predictors.
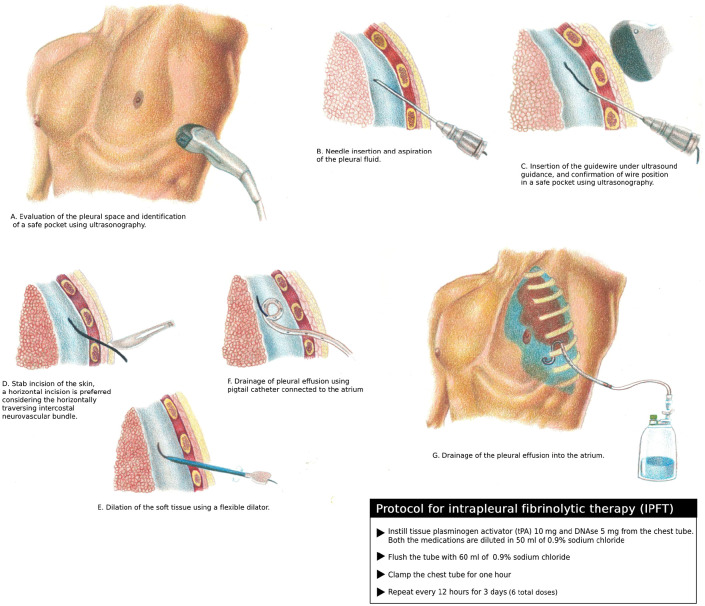
Background: Complex pleural effusion and empyema (CPPE) is treated with intrapleural fibrinolytic therapy (IPFT) using tissue plasminogen activator (tPA) and deoxyribonuclease (DNase) We present our single-center retrospective observational data using a simplified regimen of coadministering six divided doses of tPA and DNase over the course of 3 days.
Objective: To study the safety, utility, and clinical outcomes of IPFT.
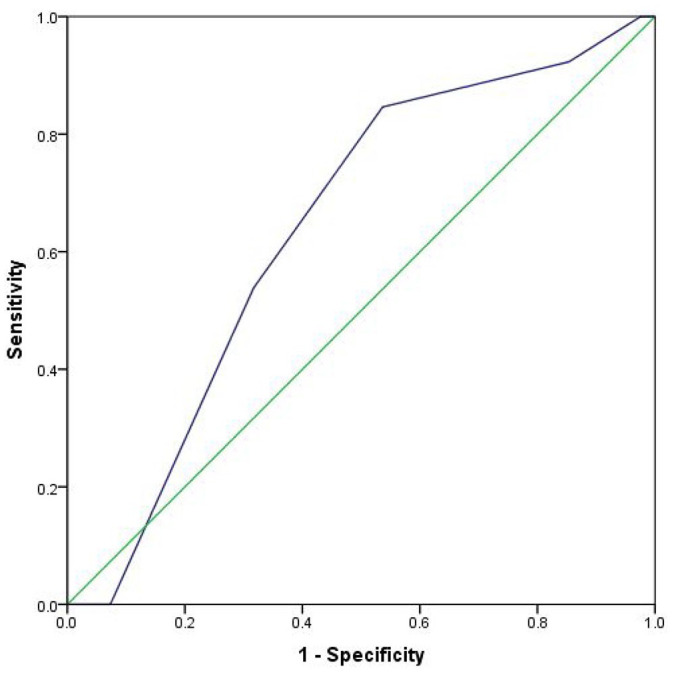
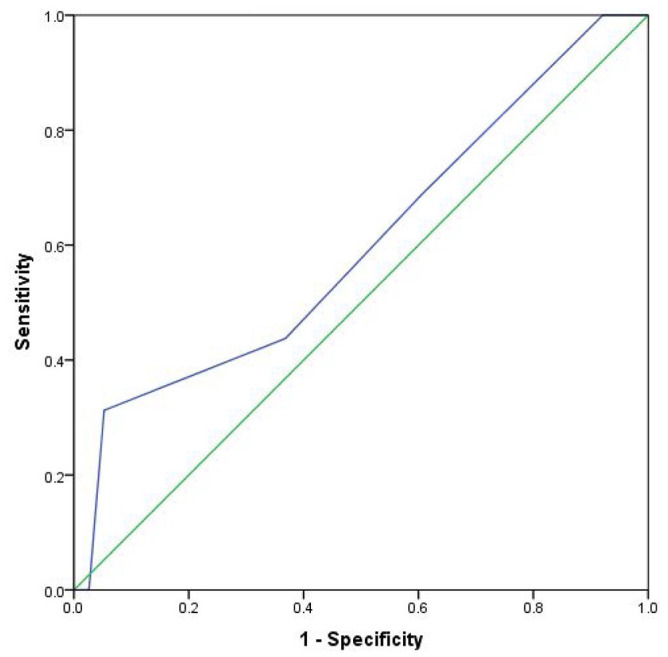
Design: This is a single-center retrospective study of patients who received co-administration tPA/DNase for CPPE over a period of 5 years. The primary outcome was successful treatment without the need for surgery. Secondary outcomes were bleeding risk, post-procedural pain, treatment complications, and all-cause mortality at 30 days and 6 months. We have tested the clinical role RAPID score (Renal function measured as urea, Age, fluid Purulence, Infection source, Dietary status measured as albumin) to predict treatment success, and all-cause mortality at 6 months.
Results: A total of (n = 55) patients were included in the study. The mean age of the population studied was 67 (Interquartile range 57-74), including 47.3% male and 52.7% Female. 92.7% of the population studied was Caucasian. Comorbidities including chronic obstructive pulmonary disease, congestive heart failure, and Diabetes mellitus were present in 41.8%, 41.8%, and 43.6.% respectively. Patients were treated with tube thoracostomy with 14 French percutaneous pigtail catheters in 47 (85.5%) or 28-32 French chest tubes in 8 (14.5%) patients. Twenty-nine percent (16) of patients had acceptable clinical and radiographic improvement and did not require additional surgical or radiological intervention. Seventy-one percent (39) of patients required additional surgical drainage; video-assisted thoracoscopic surgery in 37, and open thoracotomy in 2 patients. The discriminating ability of the RAPID score for treatment success after IPFT was found to be poor (AUC: 0.601, 95% CI: 0.429-0.773, p = 0.24). All-cause mortality at 6 months was 23.6% (13) of patients. The predictive ability of the RAPID score for mortality at 6 months was found to be poor (AUC: 0.640, 95% CI: 0.478-0.802, p = 0.13). The optimal cutoff for the RAPID score for mortality was ⩾4, with 84.6% sensitivity and 46.3% specificity.
Conclusion: Results of our single-center study suggest that IPFT can be safely adopted by small and mid-sized clinical centers, as the risk of bleeding is low. The results of coadministering tPA and DNase are safe, and it reduces the need for surgical intervention in nearly one-third of patients.
期刊介绍:
Therapeutic Advances in Respiratory Disease delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of respiratory disease.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


