Vasiliki Tsolaki, George E Zakynthinos, Nikitas Karavidas, Maria Eirini Papadonta, Ilias Dimeas, Kyriaki Parisi, Theofilos Amanatidis, Epaminondas Zakynthinos
{"title":"基于肺力学的呼气末正压滴定可改善急性呼吸窘迫综合征患者脉压变化的解释。","authors":"Vasiliki Tsolaki, George E Zakynthinos, Nikitas Karavidas, Maria Eirini Papadonta, Ilias Dimeas, Kyriaki Parisi, Theofilos Amanatidis, Epaminondas Zakynthinos","doi":"10.1097/CCE.0000000000001273","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the effects of positive end-expiratory pressure (PEEP) on pulse pressure variation (PPV) in patients with moderate/severe acute respiratory distress syndrome (ARDS).</p><p><strong>Design: </strong>Prospective interventional self-controlled study.</p><p><strong>Setting: </strong>University Hospital of Larissa.</p><p><strong>Patients: </strong>ARDS patients admitted intubated in the ICU (from August 2020 to March 2022).</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>PPV and inferior vena cava (IVC) respiratory variability were evaluated at two PEEP levels (first value mainly based on PEEP/Fio2 and second value based on respiratory system compliance). Additionally, respiratory mechanics, hemodynamics, and echocardiographic indices assessing right ventricular (RV) size (RV end-diastolic area/left ventricular end-diastolic area [RVEDA/LVEDA]), RV systolic function, and RV afterload (pulmonary artery systolic pressure [PASP] and PASP/left ventricular outflow tract velocity time integral [PASP/VTILVOT]) were recorded. Ninety-five patients were evaluated. PPV decreased after PEEP reduction (11.7 ± 0.2 to 7.9% ± 0.2%), whereas IVC respiratory variability increased (9.1 ± 0.9 to 14.6% ± 0.1%) and central venous pressure decreased (all p < 0.0001). RV afterload indices decreased (p < 0.0001), simultaneously with RV size (< 0.0001) and systolic function indices' improvements (< 0.05); shock warranted less noradrenaline doses. The change in PPV correlated significantly to respiratory variability in IVC diameter distensibility (p < 0.0001) and moderately to changes in RV size and systolic function (change in RVEDA/change in LVEDA, change in tricuspid annular plane systolic excursion); RV afterload (change in PASP [ΔPASP], ΔPASP/VTILVOT); and change in Paco2 (all p < 0.05).</p><p><strong>Conclusions: </strong>PPV alteration with PEEP decrease, associated with IVC distensibility increases, may indicate the presence of RV dysfunction and increased pulmonary vascular resistances. Whether the patients are in need for fluid loading, fluid responsiveness assessment may be further warranted.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 6","pages":"e1273"},"PeriodicalIF":2.7000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12122179/pdf/","citationCount":"0","resultStr":"{\"title\":\"Positive End-Expiratory Pressure Titration Based on Lung Mechanics May Improve Pulse Pressure Variation Interpretation in Acute Respiratory Distress Syndrome Patients.\",\"authors\":\"Vasiliki Tsolaki, George E Zakynthinos, Nikitas Karavidas, Maria Eirini Papadonta, Ilias Dimeas, Kyriaki Parisi, Theofilos Amanatidis, Epaminondas Zakynthinos\",\"doi\":\"10.1097/CCE.0000000000001273\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To evaluate the effects of positive end-expiratory pressure (PEEP) on pulse pressure variation (PPV) in patients with moderate/severe acute respiratory distress syndrome (ARDS).</p><p><strong>Design: </strong>Prospective interventional self-controlled study.</p><p><strong>Setting: </strong>University Hospital of Larissa.</p><p><strong>Patients: </strong>ARDS patients admitted intubated in the ICU (from August 2020 to March 2022).</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>PPV and inferior vena cava (IVC) respiratory variability were evaluated at two PEEP levels (first value mainly based on PEEP/Fio2 and second value based on respiratory system compliance). Additionally, respiratory mechanics, hemodynamics, and echocardiographic indices assessing right ventricular (RV) size (RV end-diastolic area/left ventricular end-diastolic area [RVEDA/LVEDA]), RV systolic function, and RV afterload (pulmonary artery systolic pressure [PASP] and PASP/left ventricular outflow tract velocity time integral [PASP/VTILVOT]) were recorded. Ninety-five patients were evaluated. PPV decreased after PEEP reduction (11.7 ± 0.2 to 7.9% ± 0.2%), whereas IVC respiratory variability increased (9.1 ± 0.9 to 14.6% ± 0.1%) and central venous pressure decreased (all p < 0.0001). RV afterload indices decreased (p < 0.0001), simultaneously with RV size (< 0.0001) and systolic function indices' improvements (< 0.05); shock warranted less noradrenaline doses. The change in PPV correlated significantly to respiratory variability in IVC diameter distensibility (p < 0.0001) and moderately to changes in RV size and systolic function (change in RVEDA/change in LVEDA, change in tricuspid annular plane systolic excursion); RV afterload (change in PASP [ΔPASP], ΔPASP/VTILVOT); and change in Paco2 (all p < 0.05).</p><p><strong>Conclusions: </strong>PPV alteration with PEEP decrease, associated with IVC distensibility increases, may indicate the presence of RV dysfunction and increased pulmonary vascular resistances. Whether the patients are in need for fluid loading, fluid responsiveness assessment may be further warranted.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 6\",\"pages\":\"e1273\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-05-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12122179/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001273\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001273","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Positive End-Expiratory Pressure Titration Based on Lung Mechanics May Improve Pulse Pressure Variation Interpretation in Acute Respiratory Distress Syndrome Patients.
Objectives: To evaluate the effects of positive end-expiratory pressure (PEEP) on pulse pressure variation (PPV) in patients with moderate/severe acute respiratory distress syndrome (ARDS).
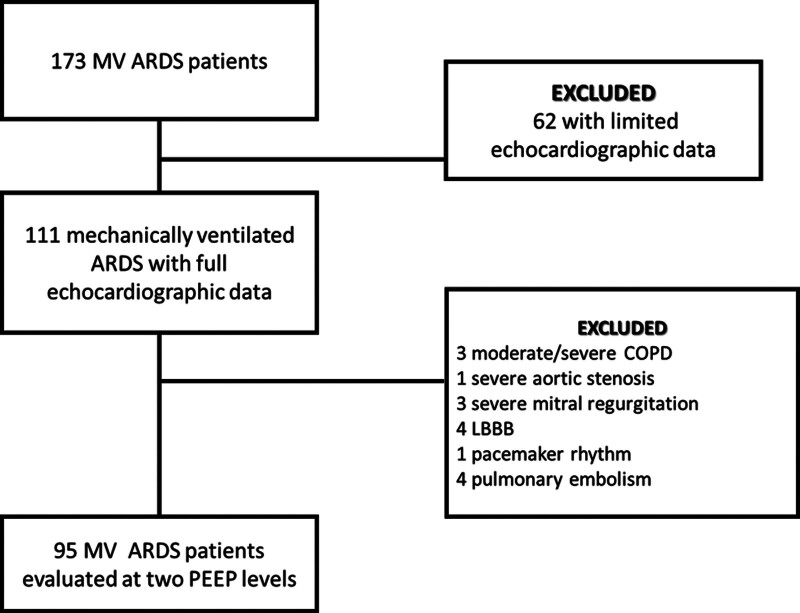
Patients: ARDS patients admitted intubated in the ICU (from August 2020 to March 2022).
Interventions: None.
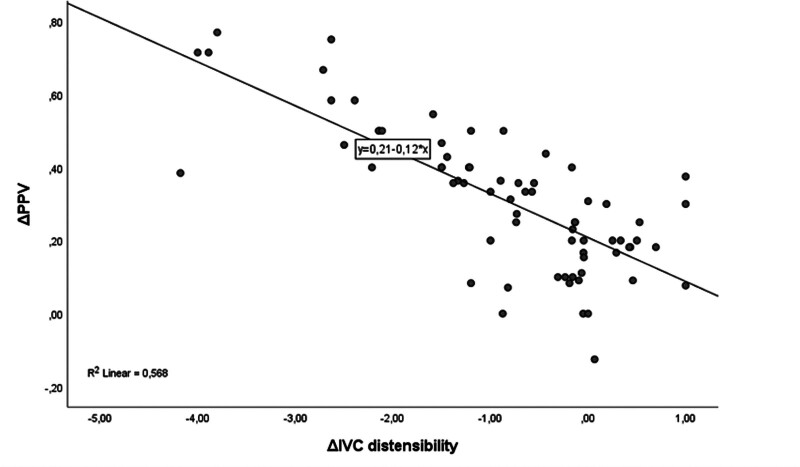
Measurements and main results: PPV and inferior vena cava (IVC) respiratory variability were evaluated at two PEEP levels (first value mainly based on PEEP/Fio2 and second value based on respiratory system compliance). Additionally, respiratory mechanics, hemodynamics, and echocardiographic indices assessing right ventricular (RV) size (RV end-diastolic area/left ventricular end-diastolic area [RVEDA/LVEDA]), RV systolic function, and RV afterload (pulmonary artery systolic pressure [PASP] and PASP/left ventricular outflow tract velocity time integral [PASP/VTILVOT]) were recorded. Ninety-five patients were evaluated. PPV decreased after PEEP reduction (11.7 ± 0.2 to 7.9% ± 0.2%), whereas IVC respiratory variability increased (9.1 ± 0.9 to 14.6% ± 0.1%) and central venous pressure decreased (all p < 0.0001). RV afterload indices decreased (p < 0.0001), simultaneously with RV size (< 0.0001) and systolic function indices' improvements (< 0.05); shock warranted less noradrenaline doses. The change in PPV correlated significantly to respiratory variability in IVC diameter distensibility (p < 0.0001) and moderately to changes in RV size and systolic function (change in RVEDA/change in LVEDA, change in tricuspid annular plane systolic excursion); RV afterload (change in PASP [ΔPASP], ΔPASP/VTILVOT); and change in Paco2 (all p < 0.05).
Conclusions: PPV alteration with PEEP decrease, associated with IVC distensibility increases, may indicate the presence of RV dysfunction and increased pulmonary vascular resistances. Whether the patients are in need for fluid loading, fluid responsiveness assessment may be further warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


