{"title":"保留射血分数的心力衰竭患者右心室功能障碍的预后意义:重建时间-事件数据的荟萃分析。","authors":"Roozbeh Narimani-Javid, Mehrdad Mahalleh, Kiyarash Behboodi, Kasra Izadpanahi, Alireza Arzhangzadeh, Reza Nikfar, Seyed Ali Hosseini, Ehsan Amini-Salehi, Sasan Shafiei, Hamed Vahidi, Kaveh Hosseini, Hamidreza Soleimani","doi":"10.1186/s44156-025-00080-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The prognosis of Heart failure with preserved ejection fraction (HFpEF) is significantly impacted by the existence and severity of comorbidities. Recent studies highlight the right ventricle (RV) as a crucial player in heart failure pathophysiology. However, there are still gaps in understanding how right ventricular dysfunction (RVD) affects long-term outcomes in patients with heart failure with preserved ejection fraction (HFpEF).</p><p><strong>Materials and methods: </strong>In this systematic review and meta-analysis, a comprehensive search was conducted to identify studies investigating RVD as the predictor of the composite outcome of All-cause death, cardiac death, and hospitalization for HF in patients with HFpEF published until October 2024. RVD was defined as the deviation of at least one measurement of RV function from the recommended normal range based on modality and the normal ranges established in each study. Time and survival probability were extracted for each Group (HFpEF patients with and without RVD) in each of the Kaplan-Meier curves. Individual patient data were reconstructed by processing the extracted time points, survival probabilities, and the number of patients at risk in a two-stage approach. The restricted mean survival time (RMST) was also calculated as the area under the survival curve for each group.</p><p><strong>Results: </strong>Seven studies met the inclusion criteria, comprising 1936 individuals, of which 555 patients had RVD. The pooled prevalence of RVD among HFpEF was 41.2% (95% CI: 36.5; 45.9). Patients with RVD had a significantly higher risk of adverse outcomes compared to those without RVD, with an HR of 2.28 (95% CI, 1.95; 2.68, p-value < 0.001) in the eight-year follow-up after the RVD diagnosis. The one-year landmark analysis revealed that the majority of the event-free survival disparity between patients with RVD and those without arises from the first year after an RVD diagnosis. Patients with RVD also had shorter event-free survival. (ΔRMST = -2.127 years, 95% CI, -2.383; -1.872, p-value < 0.001).</p><p><strong>Conclusion: </strong>The development of RVD in HFpEF is linked to significantly increased composite outcomes of all-cause death and HF hospitalization and shorter event-free survival.</p>","PeriodicalId":45749,"journal":{"name":"Echo Research and Practice","volume":"12 1","pages":"13"},"PeriodicalIF":2.4000,"publicationDate":"2025-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12121155/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic significance of right ventricular dysfunction in heart failure with preserved ejection fraction: a meta-analysis of reconstructed time-to-event data.\",\"authors\":\"Roozbeh Narimani-Javid, Mehrdad Mahalleh, Kiyarash Behboodi, Kasra Izadpanahi, Alireza Arzhangzadeh, Reza Nikfar, Seyed Ali Hosseini, Ehsan Amini-Salehi, Sasan Shafiei, Hamed Vahidi, Kaveh Hosseini, Hamidreza Soleimani\",\"doi\":\"10.1186/s44156-025-00080-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The prognosis of Heart failure with preserved ejection fraction (HFpEF) is significantly impacted by the existence and severity of comorbidities. Recent studies highlight the right ventricle (RV) as a crucial player in heart failure pathophysiology. However, there are still gaps in understanding how right ventricular dysfunction (RVD) affects long-term outcomes in patients with heart failure with preserved ejection fraction (HFpEF).</p><p><strong>Materials and methods: </strong>In this systematic review and meta-analysis, a comprehensive search was conducted to identify studies investigating RVD as the predictor of the composite outcome of All-cause death, cardiac death, and hospitalization for HF in patients with HFpEF published until October 2024. RVD was defined as the deviation of at least one measurement of RV function from the recommended normal range based on modality and the normal ranges established in each study. Time and survival probability were extracted for each Group (HFpEF patients with and without RVD) in each of the Kaplan-Meier curves. Individual patient data were reconstructed by processing the extracted time points, survival probabilities, and the number of patients at risk in a two-stage approach. The restricted mean survival time (RMST) was also calculated as the area under the survival curve for each group.</p><p><strong>Results: </strong>Seven studies met the inclusion criteria, comprising 1936 individuals, of which 555 patients had RVD. The pooled prevalence of RVD among HFpEF was 41.2% (95% CI: 36.5; 45.9). Patients with RVD had a significantly higher risk of adverse outcomes compared to those without RVD, with an HR of 2.28 (95% CI, 1.95; 2.68, p-value < 0.001) in the eight-year follow-up after the RVD diagnosis. The one-year landmark analysis revealed that the majority of the event-free survival disparity between patients with RVD and those without arises from the first year after an RVD diagnosis. Patients with RVD also had shorter event-free survival. (ΔRMST = -2.127 years, 95% CI, -2.383; -1.872, p-value < 0.001).</p><p><strong>Conclusion: </strong>The development of RVD in HFpEF is linked to significantly increased composite outcomes of all-cause death and HF hospitalization and shorter event-free survival.</p>\",\"PeriodicalId\":45749,\"journal\":{\"name\":\"Echo Research and Practice\",\"volume\":\"12 1\",\"pages\":\"13\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12121155/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Echo Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44156-025-00080-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Echo Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44156-025-00080-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Prognostic significance of right ventricular dysfunction in heart failure with preserved ejection fraction: a meta-analysis of reconstructed time-to-event data.
Background: The prognosis of Heart failure with preserved ejection fraction (HFpEF) is significantly impacted by the existence and severity of comorbidities. Recent studies highlight the right ventricle (RV) as a crucial player in heart failure pathophysiology. However, there are still gaps in understanding how right ventricular dysfunction (RVD) affects long-term outcomes in patients with heart failure with preserved ejection fraction (HFpEF).
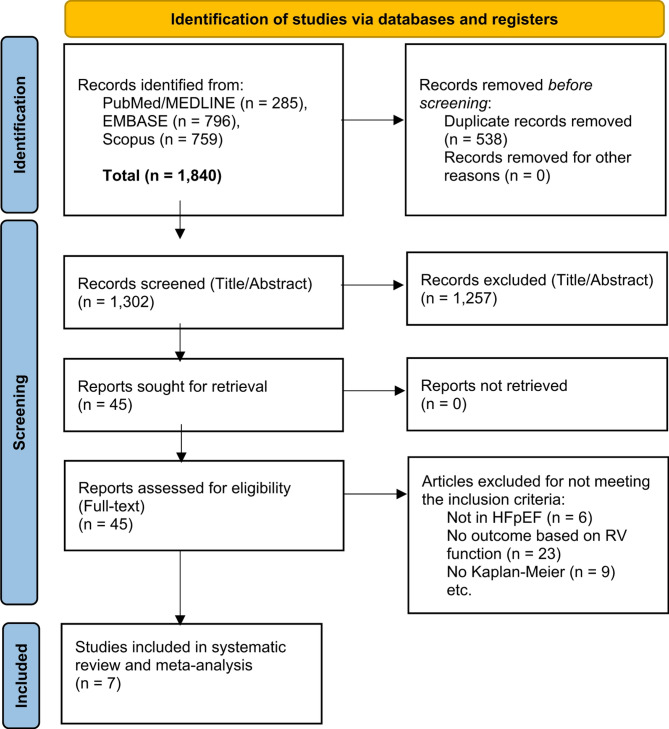
Materials and methods: In this systematic review and meta-analysis, a comprehensive search was conducted to identify studies investigating RVD as the predictor of the composite outcome of All-cause death, cardiac death, and hospitalization for HF in patients with HFpEF published until October 2024. RVD was defined as the deviation of at least one measurement of RV function from the recommended normal range based on modality and the normal ranges established in each study. Time and survival probability were extracted for each Group (HFpEF patients with and without RVD) in each of the Kaplan-Meier curves. Individual patient data were reconstructed by processing the extracted time points, survival probabilities, and the number of patients at risk in a two-stage approach. The restricted mean survival time (RMST) was also calculated as the area under the survival curve for each group.
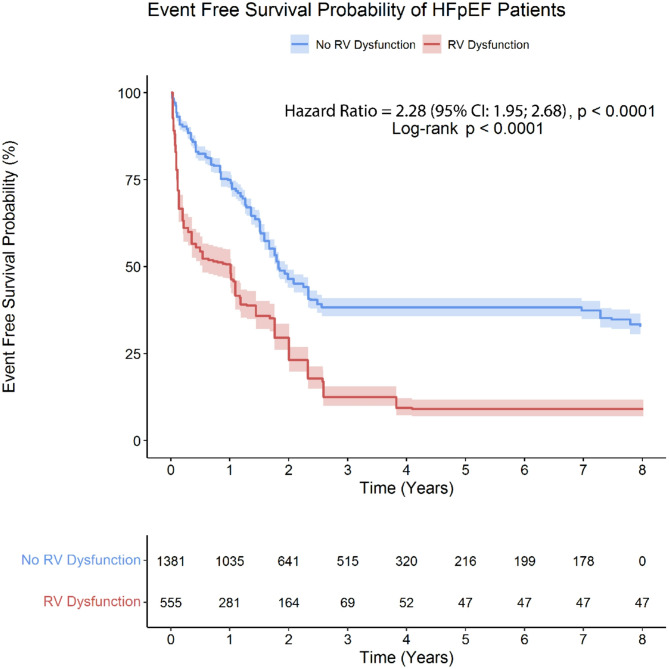
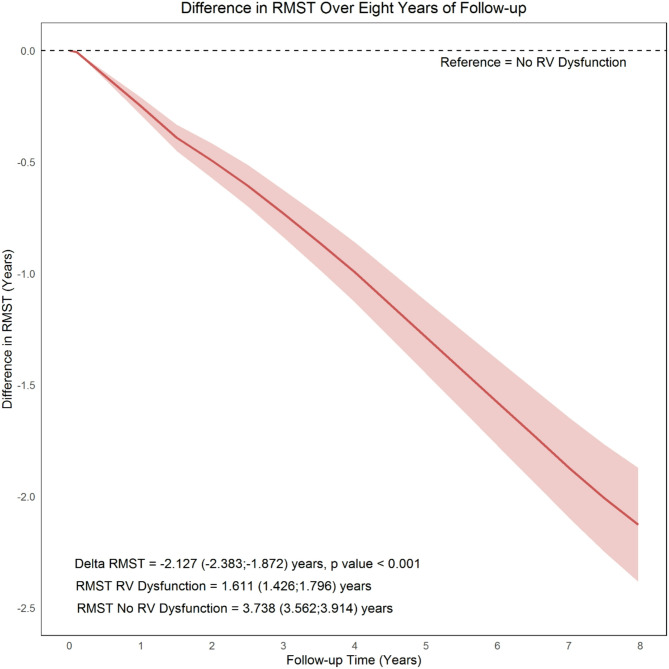
Results: Seven studies met the inclusion criteria, comprising 1936 individuals, of which 555 patients had RVD. The pooled prevalence of RVD among HFpEF was 41.2% (95% CI: 36.5; 45.9). Patients with RVD had a significantly higher risk of adverse outcomes compared to those without RVD, with an HR of 2.28 (95% CI, 1.95; 2.68, p-value < 0.001) in the eight-year follow-up after the RVD diagnosis. The one-year landmark analysis revealed that the majority of the event-free survival disparity between patients with RVD and those without arises from the first year after an RVD diagnosis. Patients with RVD also had shorter event-free survival. (ΔRMST = -2.127 years, 95% CI, -2.383; -1.872, p-value < 0.001).
Conclusion: The development of RVD in HFpEF is linked to significantly increased composite outcomes of all-cause death and HF hospitalization and shorter event-free survival.
期刊介绍:
Echo Research and Practice aims to be the premier international journal for physicians, sonographers, nurses and other allied health professionals practising echocardiography and other cardiac imaging modalities. This open-access journal publishes quality clinical and basic research, reviews, videos, education materials and selected high-interest case reports and videos across all echocardiography modalities and disciplines, including paediatrics, anaesthetics, general practice, acute medicine and intensive care. Multi-modality studies primarily featuring the use of cardiac ultrasound in clinical practice, in association with Cardiac Computed Tomography, Cardiovascular Magnetic Resonance or Nuclear Cardiology are of interest. Topics include, but are not limited to: 2D echocardiography 3D echocardiography Comparative imaging techniques – CCT, CMR and Nuclear Cardiology Congenital heart disease, including foetal echocardiography Contrast echocardiography Critical care echocardiography Deformation imaging Doppler echocardiography Interventional echocardiography Intracardiac echocardiography Intraoperative echocardiography Prosthetic valves Stress echocardiography Technical innovations Transoesophageal echocardiography Valve disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


