Ji Hoon Bahk, Joo-Hyoun Song, Young Wook Lim, Cheolsoon Park, Kee-Haeng Lee
{"title":"一期无骨水泥全髋关节置换术治疗股骨头坏死导致的快速破坏性骨关节病的疗效:一项匹配队列研究。","authors":"Ji Hoon Bahk, Joo-Hyoun Song, Young Wook Lim, Cheolsoon Park, Kee-Haeng Lee","doi":"10.5371/hp.2025.37.2.112","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Total hip arthroplasty (THA) is the only definitive treatment for rapidly destructive coxarthrosis (RDC). THA for RDC has significantly higher perioperative blood loss with a greater requirement for transfusion than non-RDC primary THAs. Given the rarity of the disease, this study aimed to investigate perioperative and long-term outcomes of cementless THA for RDC that developed from osteonecrosis of the femoral head (ONFH).</p><p><strong>Materials and methods: </strong>Each of 26 RDC patients was matched to a patient with typical advanced-stage ONFH for comparison, according to age, sex, American Society of Anesthesiologists classification, and the type of implant used. As a primary outcome, perioperative blood loss was calculated as the sum of compensated and uncompensated blood loss.</p><p><strong>Results: </strong>The RDC group had a significantly larger amount of total perioperative blood loss in comparison to the group with typical ONFH (791.5 mL vs. 511.2 mL, <i>P</i>=0.034), which was primarily attributable to compensated blood loss (496.1 mL vs. 141.5 mL, <i>P</i>=0.024), as uncompensated blood loss was not significantly different (<i>P</i>=0.152). Intraoperative transfusion volume was significantly higher in the RDC group (234.6 mL vs. 46.2 mL, <i>P</i>=0.007), while the difference in postoperative transfusion was marginally significant (<i>P</i>=0.092).</p><p><strong>Conclusion: </strong>THA for RDC was accompanied by a higher perioperative blood loss, attributable mainly to a significant difference in the amount of intraoperative transfusion, in a matched comparison with patients with typical advanced-stage ONFH. However, extended operation time and prolonged hospitalization along with a large volume of transfusion did not translate into inferior long-term outcomes.</p>","PeriodicalId":73239,"journal":{"name":"Hip & pelvis","volume":"37 2","pages":"112-119"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12120481/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes of Primary Cementless Total Hip Arthroplasty for Rapidly Destructive Coxarthrosis from Osteonecrosis of the Femoral Head: A Matched Cohort Study.\",\"authors\":\"Ji Hoon Bahk, Joo-Hyoun Song, Young Wook Lim, Cheolsoon Park, Kee-Haeng Lee\",\"doi\":\"10.5371/hp.2025.37.2.112\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Total hip arthroplasty (THA) is the only definitive treatment for rapidly destructive coxarthrosis (RDC). THA for RDC has significantly higher perioperative blood loss with a greater requirement for transfusion than non-RDC primary THAs. Given the rarity of the disease, this study aimed to investigate perioperative and long-term outcomes of cementless THA for RDC that developed from osteonecrosis of the femoral head (ONFH).</p><p><strong>Materials and methods: </strong>Each of 26 RDC patients was matched to a patient with typical advanced-stage ONFH for comparison, according to age, sex, American Society of Anesthesiologists classification, and the type of implant used. As a primary outcome, perioperative blood loss was calculated as the sum of compensated and uncompensated blood loss.</p><p><strong>Results: </strong>The RDC group had a significantly larger amount of total perioperative blood loss in comparison to the group with typical ONFH (791.5 mL vs. 511.2 mL, <i>P</i>=0.034), which was primarily attributable to compensated blood loss (496.1 mL vs. 141.5 mL, <i>P</i>=0.024), as uncompensated blood loss was not significantly different (<i>P</i>=0.152). Intraoperative transfusion volume was significantly higher in the RDC group (234.6 mL vs. 46.2 mL, <i>P</i>=0.007), while the difference in postoperative transfusion was marginally significant (<i>P</i>=0.092).</p><p><strong>Conclusion: </strong>THA for RDC was accompanied by a higher perioperative blood loss, attributable mainly to a significant difference in the amount of intraoperative transfusion, in a matched comparison with patients with typical advanced-stage ONFH. However, extended operation time and prolonged hospitalization along with a large volume of transfusion did not translate into inferior long-term outcomes.</p>\",\"PeriodicalId\":73239,\"journal\":{\"name\":\"Hip & pelvis\",\"volume\":\"37 2\",\"pages\":\"112-119\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12120481/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hip & pelvis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5371/hp.2025.37.2.112\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hip & pelvis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5371/hp.2025.37.2.112","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:全髋关节置换术(THA)是快速破坏性关节(RDC)的唯一确定治疗方法。与非RDC原发性THA相比,RDC的THA围手术期出血量明显更高,输血需求也更大。鉴于这种疾病的罕见性,本研究旨在探讨无骨水泥THA治疗股骨头坏死(ONFH)所致RDC的围手术期和长期预后。材料和方法:根据年龄、性别、美国麻醉学会分类和使用的植入物类型,将26例RDC患者与1例典型的晚期ONFH患者进行匹配进行比较。围手术期失血量计算为代偿失血量和非代偿失血量之和。结果:RDC组围手术期总失血量明显大于典型ONFH组(791.5 mL比511.2 mL, P=0.034),主要为代偿失血量(496.1 mL比141.5 mL, P=0.024),非代偿失血量差异无统计学意义(P=0.152)。RDC组术中输血量显著高于RDC组(234.6 mL vs. 46.2 mL, P=0.007),术后输血量差异无统计学意义(P=0.092)。结论:与典型晚期ONFH患者相比,RDC THA患者围术期出血量较高,主要原因是术中输血量存在显著差异。然而,手术时间的延长和住院时间的延长以及大量输血并不意味着长期预后较差。
Outcomes of Primary Cementless Total Hip Arthroplasty for Rapidly Destructive Coxarthrosis from Osteonecrosis of the Femoral Head: A Matched Cohort Study.
Purpose: Total hip arthroplasty (THA) is the only definitive treatment for rapidly destructive coxarthrosis (RDC). THA for RDC has significantly higher perioperative blood loss with a greater requirement for transfusion than non-RDC primary THAs. Given the rarity of the disease, this study aimed to investigate perioperative and long-term outcomes of cementless THA for RDC that developed from osteonecrosis of the femoral head (ONFH).
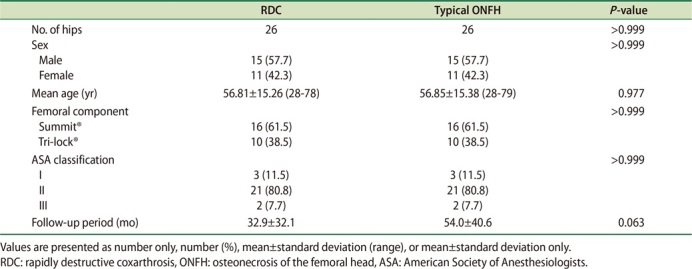
Materials and methods: Each of 26 RDC patients was matched to a patient with typical advanced-stage ONFH for comparison, according to age, sex, American Society of Anesthesiologists classification, and the type of implant used. As a primary outcome, perioperative blood loss was calculated as the sum of compensated and uncompensated blood loss.
Results: The RDC group had a significantly larger amount of total perioperative blood loss in comparison to the group with typical ONFH (791.5 mL vs. 511.2 mL, P=0.034), which was primarily attributable to compensated blood loss (496.1 mL vs. 141.5 mL, P=0.024), as uncompensated blood loss was not significantly different (P=0.152). Intraoperative transfusion volume was significantly higher in the RDC group (234.6 mL vs. 46.2 mL, P=0.007), while the difference in postoperative transfusion was marginally significant (P=0.092).
Conclusion: THA for RDC was accompanied by a higher perioperative blood loss, attributable mainly to a significant difference in the amount of intraoperative transfusion, in a matched comparison with patients with typical advanced-stage ONFH. However, extended operation time and prolonged hospitalization along with a large volume of transfusion did not translate into inferior long-term outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


