Michelle T Martin, Krithika Rajagopalan, Dilip Makhija, Fatema Turkistani, Caroline Burk, Marvin Rock, Alice Hsiao, Nancy Reau
{"title":"美国医疗补助对直接作用的丙型肝炎病毒抗病毒药物限制相关的卫生保健资源利用和成本:回顾性索赔数据库分析","authors":"Michelle T Martin, Krithika Rajagopalan, Dilip Makhija, Fatema Turkistani, Caroline Burk, Marvin Rock, Alice Hsiao, Nancy Reau","doi":"10.1007/s40273-025-01487-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Many state Medicaid programs implemented sobriety restrictions that delay timely initiation of direct-acting antivirals (DAAs) for patients with hepatitis C virus (HCV) infections. This claims database study examined the economic impact of sobriety restrictions on DAAs among Medicaid-insured patients with HCV.</p><p><strong>Methods: </strong>A retrospective database analysis of the Anlitiks All Payor Claims data (APCD) during the period January 1, 2020 to June 30, 2022 was conducted. Continuously enrolled adult (aged 18-64 years) Medicaid-insured patients with HCV who initiated DAAs (i.e., index date) during the period January 1, 2021 to December 31, 2021 with ≥ 12 months pre-index and ≥ 6 months post-index follow-up were categorized into two cohorts (states with sobriety restriction [SR] and states with no sobriety restriction [NSR]) based on the sobriety restriction status in the state of residence on the index date. Measures analyzed were the proportion of patients with one or more all-cause medical health care resource utilization (HCRU) (inpatient hospitalization [IP], emergency department [ED], outpatient [OP], professional office [PV], and other [OV] visits) and mean per-patient medical, pharmacy, and overall costs. HCRU and cost differences were compared using adjusted multivariable logistic and gamma-log link regression models, respectively.</p><p><strong>Results: </strong>Patients in the SR (n = 2,295) versus NSR (n = 4,623) cohort had a higher mean age (45 ± 12.02 vs. 43 ± 11.51 years), fewer males (50.28% vs. 58.1%), and they had lower substance use rates (44.10% vs. 59.68%), all significant at p < 0.05. The SR vs. NSR cohort had higher rates of patients with all-cause HCRU by type (IP 22.0% vs.18.1%; ED 42.3% vs. 37.4; OP 62.5% vs. 55.4%; PV 76.4% vs. 69.1%; other visits 47.4% vs. 46.5%). The SR vs. NSR cohort had a significantly higher adjusted odds ratio (95% confidence interval) for IP (2.09; 1.59-2.73) and OP (1.52; 1.28-1.82). Similarly, the SR versus NSR cohort had a significantly higher all-cause adjusted least squares mean cost per patient for IP ($42,616 vs. $15,063), ED ($982 vs. $420), OP ($715 vs. $349), PV ($840 vs. $621), medical ($11,845 vs. $3,850), pharmacy ($53,453 vs. $38,298), and overall ($63,935 vs. $41,524).</p><p><strong>Conclusion: </strong>Patients who initiated DAAs with SR versus NSR had 2 times and 1.5 times greater likelihood of IP and OP visits, respectively. Similarly, the SR versus NSR cohort had 3 times greater medical costs. Restricting DAA access among patients with HCV increases HCRU and cost burden, potentially impeding World Health Organization (WHO) 2030 HCV global elimination goals.</p>","PeriodicalId":19807,"journal":{"name":"PharmacoEconomics","volume":" ","pages":"1109-1122"},"PeriodicalIF":4.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12370557/pdf/","citationCount":"0","resultStr":"{\"title\":\"Health Care Resource Utilization and Costs Associated with US Medicaid Sobriety Restrictions on Direct-Acting Antivirals for Hepatitis C Virus: A Retrospective Claims Database Analysis.\",\"authors\":\"Michelle T Martin, Krithika Rajagopalan, Dilip Makhija, Fatema Turkistani, Caroline Burk, Marvin Rock, Alice Hsiao, Nancy Reau\",\"doi\":\"10.1007/s40273-025-01487-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and aims: </strong>Many state Medicaid programs implemented sobriety restrictions that delay timely initiation of direct-acting antivirals (DAAs) for patients with hepatitis C virus (HCV) infections. This claims database study examined the economic impact of sobriety restrictions on DAAs among Medicaid-insured patients with HCV.</p><p><strong>Methods: </strong>A retrospective database analysis of the Anlitiks All Payor Claims data (APCD) during the period January 1, 2020 to June 30, 2022 was conducted. Continuously enrolled adult (aged 18-64 years) Medicaid-insured patients with HCV who initiated DAAs (i.e., index date) during the period January 1, 2021 to December 31, 2021 with ≥ 12 months pre-index and ≥ 6 months post-index follow-up were categorized into two cohorts (states with sobriety restriction [SR] and states with no sobriety restriction [NSR]) based on the sobriety restriction status in the state of residence on the index date. Measures analyzed were the proportion of patients with one or more all-cause medical health care resource utilization (HCRU) (inpatient hospitalization [IP], emergency department [ED], outpatient [OP], professional office [PV], and other [OV] visits) and mean per-patient medical, pharmacy, and overall costs. HCRU and cost differences were compared using adjusted multivariable logistic and gamma-log link regression models, respectively.</p><p><strong>Results: </strong>Patients in the SR (n = 2,295) versus NSR (n = 4,623) cohort had a higher mean age (45 ± 12.02 vs. 43 ± 11.51 years), fewer males (50.28% vs. 58.1%), and they had lower substance use rates (44.10% vs. 59.68%), all significant at p < 0.05. The SR vs. NSR cohort had higher rates of patients with all-cause HCRU by type (IP 22.0% vs.18.1%; ED 42.3% vs. 37.4; OP 62.5% vs. 55.4%; PV 76.4% vs. 69.1%; other visits 47.4% vs. 46.5%). The SR vs. NSR cohort had a significantly higher adjusted odds ratio (95% confidence interval) for IP (2.09; 1.59-2.73) and OP (1.52; 1.28-1.82). Similarly, the SR versus NSR cohort had a significantly higher all-cause adjusted least squares mean cost per patient for IP ($42,616 vs. $15,063), ED ($982 vs. $420), OP ($715 vs. $349), PV ($840 vs. $621), medical ($11,845 vs. $3,850), pharmacy ($53,453 vs. $38,298), and overall ($63,935 vs. $41,524).</p><p><strong>Conclusion: </strong>Patients who initiated DAAs with SR versus NSR had 2 times and 1.5 times greater likelihood of IP and OP visits, respectively. Similarly, the SR versus NSR cohort had 3 times greater medical costs. Restricting DAA access among patients with HCV increases HCRU and cost burden, potentially impeding World Health Organization (WHO) 2030 HCV global elimination goals.</p>\",\"PeriodicalId\":19807,\"journal\":{\"name\":\"PharmacoEconomics\",\"volume\":\" \",\"pages\":\"1109-1122\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12370557/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PharmacoEconomics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40273-025-01487-y\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40273-025-01487-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/28 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:许多州的医疗补助计划实施了清醒限制,延迟了丙型肝炎病毒(HCV)感染患者及时启动直接作用抗病毒药物(DAAs)。本索赔数据库研究考察了在HCV医疗保险患者中,清醒限制对daa的经济影响。方法:对2020年1月1日至2022年6月30日期间的anlitks所有付款人索赔数据(APCD)进行回顾性数据库分析。在2021年1月1日至2021年12月31日期间(即指数日)开始DAAs的持续入组的成人(18-64岁)医疗保险参保HCV患者,在指数前随访≥12个月,指数后随访≥6个月,根据指数日居住州的清醒限制状况分为有清醒限制州(SR)和无清醒限制州(NSR)两组。分析的指标包括一次或多次全因医疗保健资源利用率(HCRU)(住院[IP]、急诊科[ED]、门诊[OP]、专业办公室[PV]和其他[OV]就诊)的患者比例,以及每位患者的平均医疗费用、药费和总费用。HCRU和成本差异分别使用调整后的多变量logistic和γ -log链接回归模型进行比较。结果:SR组(n = 2295)与NSR组(n = 4623)患者的平均年龄(45±12.02岁vs. 43±11.51岁)较高,男性较少(50.28% vs. 58.1%),物质使用率较低(44.10% vs. 59.68%), p均具有显著性差异。结论:与NSR组相比,SR组开始daa的患者出现IP和OP就诊的可能性分别是SR组的2倍和1.5倍。同样,SR组的医疗费用是NSR组的3倍。限制HCV患者获得DAA会增加HCRU和成本负担,可能阻碍世界卫生组织(WHO) 2030年全球消除HCV的目标。
Health Care Resource Utilization and Costs Associated with US Medicaid Sobriety Restrictions on Direct-Acting Antivirals for Hepatitis C Virus: A Retrospective Claims Database Analysis.
Background and aims: Many state Medicaid programs implemented sobriety restrictions that delay timely initiation of direct-acting antivirals (DAAs) for patients with hepatitis C virus (HCV) infections. This claims database study examined the economic impact of sobriety restrictions on DAAs among Medicaid-insured patients with HCV.
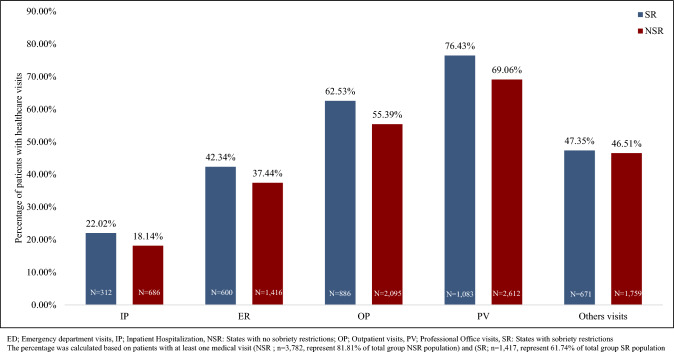
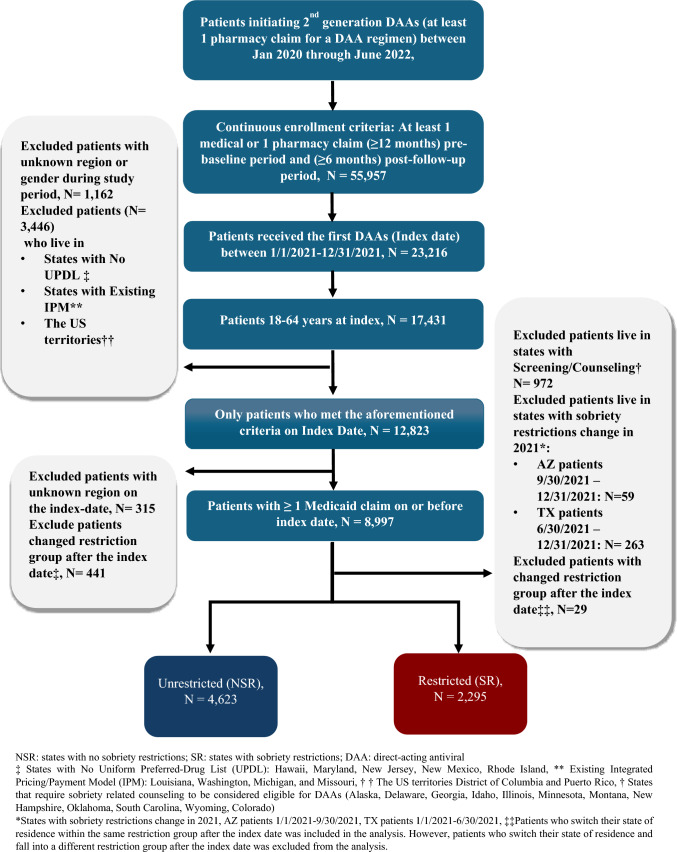
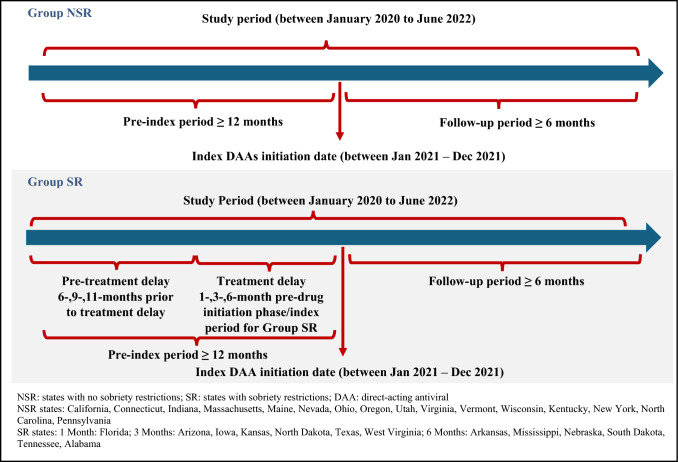
Methods: A retrospective database analysis of the Anlitiks All Payor Claims data (APCD) during the period January 1, 2020 to June 30, 2022 was conducted. Continuously enrolled adult (aged 18-64 years) Medicaid-insured patients with HCV who initiated DAAs (i.e., index date) during the period January 1, 2021 to December 31, 2021 with ≥ 12 months pre-index and ≥ 6 months post-index follow-up were categorized into two cohorts (states with sobriety restriction [SR] and states with no sobriety restriction [NSR]) based on the sobriety restriction status in the state of residence on the index date. Measures analyzed were the proportion of patients with one or more all-cause medical health care resource utilization (HCRU) (inpatient hospitalization [IP], emergency department [ED], outpatient [OP], professional office [PV], and other [OV] visits) and mean per-patient medical, pharmacy, and overall costs. HCRU and cost differences were compared using adjusted multivariable logistic and gamma-log link regression models, respectively.
Results: Patients in the SR (n = 2,295) versus NSR (n = 4,623) cohort had a higher mean age (45 ± 12.02 vs. 43 ± 11.51 years), fewer males (50.28% vs. 58.1%), and they had lower substance use rates (44.10% vs. 59.68%), all significant at p < 0.05. The SR vs. NSR cohort had higher rates of patients with all-cause HCRU by type (IP 22.0% vs.18.1%; ED 42.3% vs. 37.4; OP 62.5% vs. 55.4%; PV 76.4% vs. 69.1%; other visits 47.4% vs. 46.5%). The SR vs. NSR cohort had a significantly higher adjusted odds ratio (95% confidence interval) for IP (2.09; 1.59-2.73) and OP (1.52; 1.28-1.82). Similarly, the SR versus NSR cohort had a significantly higher all-cause adjusted least squares mean cost per patient for IP ($42,616 vs. $15,063), ED ($982 vs. $420), OP ($715 vs. $349), PV ($840 vs. $621), medical ($11,845 vs. $3,850), pharmacy ($53,453 vs. $38,298), and overall ($63,935 vs. $41,524).
Conclusion: Patients who initiated DAAs with SR versus NSR had 2 times and 1.5 times greater likelihood of IP and OP visits, respectively. Similarly, the SR versus NSR cohort had 3 times greater medical costs. Restricting DAA access among patients with HCV increases HCRU and cost burden, potentially impeding World Health Organization (WHO) 2030 HCV global elimination goals.
期刊介绍:
PharmacoEconomics is the benchmark journal for peer-reviewed, authoritative and practical articles on the application of pharmacoeconomics and quality-of-life assessment to optimum drug therapy and health outcomes. An invaluable source of applied pharmacoeconomic original research and educational material for the healthcare decision maker.
PharmacoEconomics is dedicated to the clear communication of complex pharmacoeconomic issues related to patient care and drug utilization.
PharmacoEconomics offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by a Key Points summary, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


