{"title":"危重休克患者个体化血压目标与标准治疗的多中心随机对照试验","authors":"Rakshit Panwar, Bairbre McNicholas, Ciprian Nita, Alison Gibberd, Amber-Louise Poulter, Marcia Tauares, Lauren Ferguson","doi":"10.1186/s40560-025-00798-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Minimizing relative hypotension, or mean arterial pressure (MAP) deficit, by targeting patients' own pre-illness MAP (individualized MAP) during vasopressor therapy is a potential strategy to improve outcomes among ICU patients with shock. We conducted a prospective, open label, parallel-group, pilot RCT to assess feasibility and safety of this intervention compared to standard care.</p><p><strong>Methods: </strong>Thirty-seven eligible patients, aged 40 years or older and receiving vasopressor support for shock, were randomly allocated to individualized MAP target (N = 17) or standard MAP target (N = 20) at two multidisciplinary ICUs in Australia and Ireland. Pre-specified endpoints were time-weighted average MAP-deficit (i.e., percentage difference between patients' pre-illness MAP and achieved-MAP), percentage time spent with > 20% MAP-deficit, major adverse kidney events (MAKE-14), 14-day and 90-day all-cause mortality, and cardiovascular adverse events within 28 days of randomization. All comparisons of efficacy outcomes were exploratory.</p><p><strong>Results: </strong>The median MAP-deficit and percentage time with > 20% MAP-deficit with individualized MAP vs. standard MAP were 7% [interquartile range: 2-16] vs. 18% [9-23] (p = 0.048), and 8% [0-43] vs. 53% [14-75] (p = 0.03), respectively. MAKE-14 (2/17 (12%) vs. 4/20 (20%), p = 0.67), 14-day mortality (1/17 (6%) vs. 3/20 (15%), p = 0.61), 90-day mortality (2/17 (12%) vs. 4/20 (20%), p = 0.67) and cardiovascular adverse events were similar for both groups.</p><p><strong>Conclusions: </strong>This pilot RCT demonstrated that an individualized MAP target strategy was feasible to implement. No adverse safety signals were evident. These data and study procedures helped inform the design of a definitive RCT on the question of individualized MAP targets among critically ill patients with shock.</p><p><strong>Study registration: </strong>ACTRN12618000571279.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"13 1","pages":"29"},"PeriodicalIF":4.7000,"publicationDate":"2025-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12107948/pdf/","citationCount":"0","resultStr":"{\"title\":\"A pilot multicenter randomized controlled trial on individualized blood pressure targets versus standard care among critically ill patients with shock.\",\"authors\":\"Rakshit Panwar, Bairbre McNicholas, Ciprian Nita, Alison Gibberd, Amber-Louise Poulter, Marcia Tauares, Lauren Ferguson\",\"doi\":\"10.1186/s40560-025-00798-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Minimizing relative hypotension, or mean arterial pressure (MAP) deficit, by targeting patients' own pre-illness MAP (individualized MAP) during vasopressor therapy is a potential strategy to improve outcomes among ICU patients with shock. We conducted a prospective, open label, parallel-group, pilot RCT to assess feasibility and safety of this intervention compared to standard care.</p><p><strong>Methods: </strong>Thirty-seven eligible patients, aged 40 years or older and receiving vasopressor support for shock, were randomly allocated to individualized MAP target (N = 17) or standard MAP target (N = 20) at two multidisciplinary ICUs in Australia and Ireland. Pre-specified endpoints were time-weighted average MAP-deficit (i.e., percentage difference between patients' pre-illness MAP and achieved-MAP), percentage time spent with > 20% MAP-deficit, major adverse kidney events (MAKE-14), 14-day and 90-day all-cause mortality, and cardiovascular adverse events within 28 days of randomization. All comparisons of efficacy outcomes were exploratory.</p><p><strong>Results: </strong>The median MAP-deficit and percentage time with > 20% MAP-deficit with individualized MAP vs. standard MAP were 7% [interquartile range: 2-16] vs. 18% [9-23] (p = 0.048), and 8% [0-43] vs. 53% [14-75] (p = 0.03), respectively. MAKE-14 (2/17 (12%) vs. 4/20 (20%), p = 0.67), 14-day mortality (1/17 (6%) vs. 3/20 (15%), p = 0.61), 90-day mortality (2/17 (12%) vs. 4/20 (20%), p = 0.67) and cardiovascular adverse events were similar for both groups.</p><p><strong>Conclusions: </strong>This pilot RCT demonstrated that an individualized MAP target strategy was feasible to implement. No adverse safety signals were evident. These data and study procedures helped inform the design of a definitive RCT on the question of individualized MAP targets among critically ill patients with shock.</p><p><strong>Study registration: </strong>ACTRN12618000571279.</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"13 1\",\"pages\":\"29\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2025-05-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12107948/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-025-00798-8\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-025-00798-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:在血管加压治疗期间,通过针对患者自身病前MAP(个体化MAP)来减少相对低血压或平均动脉压(MAP)缺陷是改善ICU休克患者预后的潜在策略。我们进行了一项前瞻性、开放标签、平行组、先导随机对照试验,以评估与标准治疗相比,该干预措施的可行性和安全性。方法:37例符合条件的患者,年龄在40岁及以上,接受血管加压药物支持治疗休克,随机分配到澳大利亚和爱尔兰两个多学科icu的个体化MAP靶(N = 17)或标准MAP靶(N = 20)。预先指定的终点是时间加权平均MAP缺陷(即患者病前MAP与实现MAP之间的百分比差异),> 20% MAP缺陷的时间百分比,主要不良肾脏事件(MAKE-14), 14天和90天的全因死亡率,以及随机化28天内的心血管不良事件。所有疗效结果的比较都是探索性的。结果:个体化MAP与标准MAP的中位MAP缺陷和20% MAP缺陷的时间百分比分别为7%[四分位数范围:2-16]和18% [9-23](p = 0.048), 8%[0-43]和53% [14-75](p = 0.03)。两组的MAKE-14 (2/17 (12%) vs. 4/20 (20%), p = 0.67)、14天死亡率(1/17 (6%)vs. 3/20 (15%), p = 0.61)、90天死亡率(2/17 (12%)vs. 4/20 (20%), p = 0.67)和心血管不良事件相似。结论:该试验RCT证明了个体化MAP目标策略是可行的。没有明显的不利安全信号。这些数据和研究程序有助于设计一项明确的随机对照试验,探讨危重休克患者个体化MAP靶点的问题。研究注册:ACTRN12618000571279。
A pilot multicenter randomized controlled trial on individualized blood pressure targets versus standard care among critically ill patients with shock.
Background: Minimizing relative hypotension, or mean arterial pressure (MAP) deficit, by targeting patients' own pre-illness MAP (individualized MAP) during vasopressor therapy is a potential strategy to improve outcomes among ICU patients with shock. We conducted a prospective, open label, parallel-group, pilot RCT to assess feasibility and safety of this intervention compared to standard care.
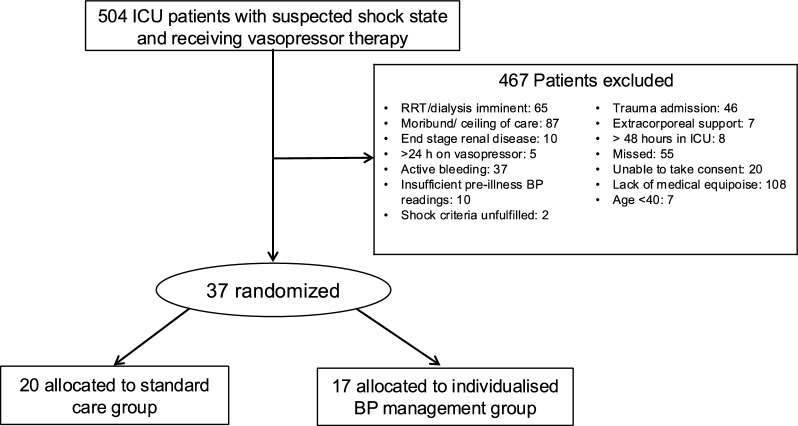
Methods: Thirty-seven eligible patients, aged 40 years or older and receiving vasopressor support for shock, were randomly allocated to individualized MAP target (N = 17) or standard MAP target (N = 20) at two multidisciplinary ICUs in Australia and Ireland. Pre-specified endpoints were time-weighted average MAP-deficit (i.e., percentage difference between patients' pre-illness MAP and achieved-MAP), percentage time spent with > 20% MAP-deficit, major adverse kidney events (MAKE-14), 14-day and 90-day all-cause mortality, and cardiovascular adverse events within 28 days of randomization. All comparisons of efficacy outcomes were exploratory.
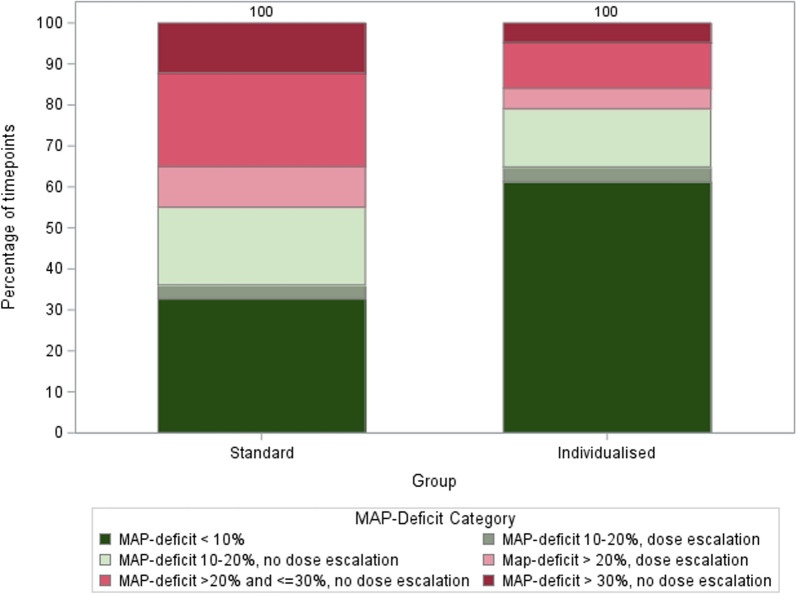
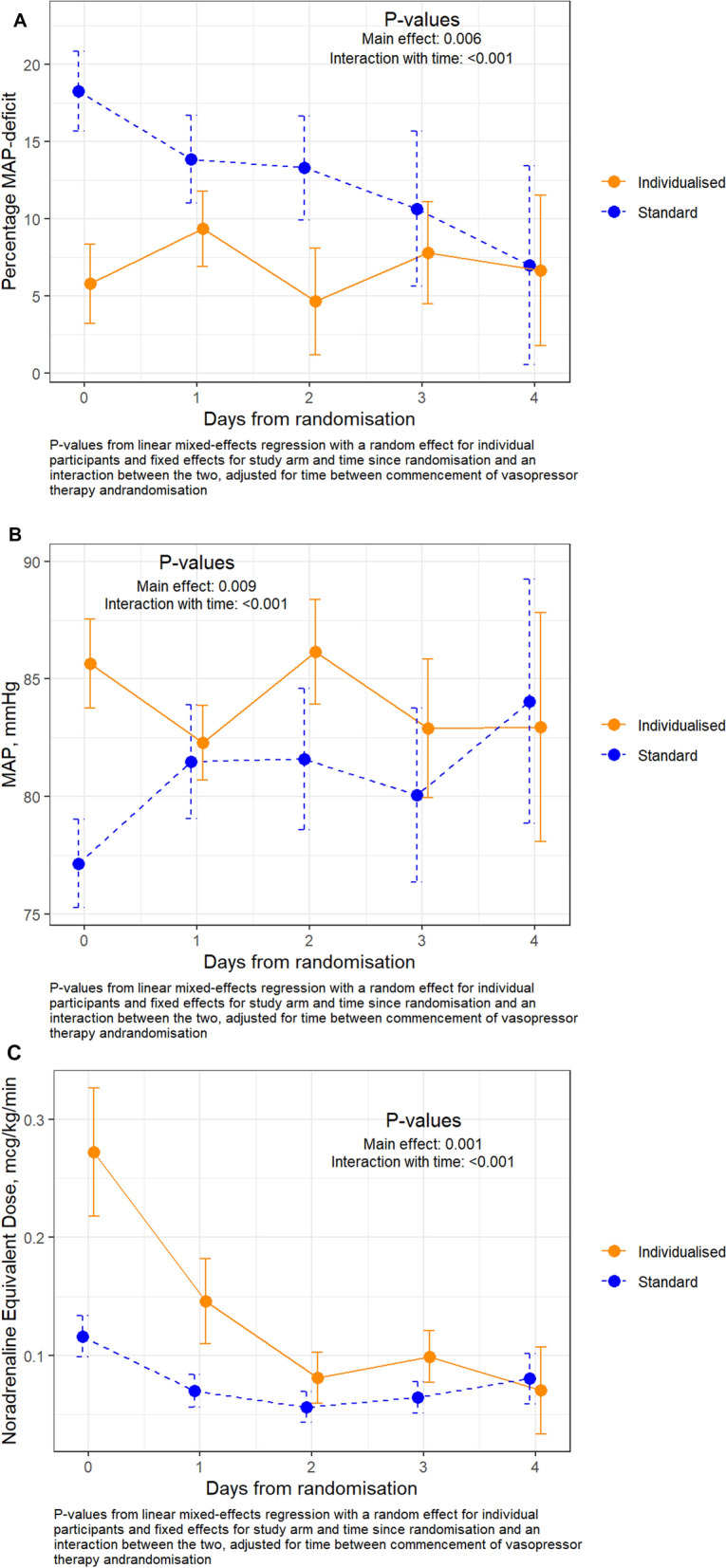
Results: The median MAP-deficit and percentage time with > 20% MAP-deficit with individualized MAP vs. standard MAP were 7% [interquartile range: 2-16] vs. 18% [9-23] (p = 0.048), and 8% [0-43] vs. 53% [14-75] (p = 0.03), respectively. MAKE-14 (2/17 (12%) vs. 4/20 (20%), p = 0.67), 14-day mortality (1/17 (6%) vs. 3/20 (15%), p = 0.61), 90-day mortality (2/17 (12%) vs. 4/20 (20%), p = 0.67) and cardiovascular adverse events were similar for both groups.
Conclusions: This pilot RCT demonstrated that an individualized MAP target strategy was feasible to implement. No adverse safety signals were evident. These data and study procedures helped inform the design of a definitive RCT on the question of individualized MAP targets among critically ill patients with shock.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


