Mazyad M Alenezi, Faisal A Al-Harbi, Albaraa Nasser M Almoshigeh, Sultan S Alruqaie, Nada M Alshahrani, Alwaleed Mohammed Alamro, Abdulmalik Abdulaziz Aljulajil, Rayan Abduallah Alsaqri, Lama A Alharbi
{"title":"不同扁桃体切除技术后出血率的比较:系统回顾和Meta分析。","authors":"Mazyad M Alenezi, Faisal A Al-Harbi, Albaraa Nasser M Almoshigeh, Sultan S Alruqaie, Nada M Alshahrani, Alwaleed Mohammed Alamro, Abdulmalik Abdulaziz Aljulajil, Rayan Abduallah Alsaqri, Lama A Alharbi","doi":"10.3390/clinpract15050085","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b>: Post-tonsillectomy hemorrhage is a serious complication that varies according to the surgical technique used, potentially compromising patient safety and recovery. Even though several techniques were frequently used, including cold steel dissection, coblation, monopolar diathermy, and bipolar diathermy, there were certain discrepancies in hemorrhage rates in the literature. This meta-analysis aims to compare the rates of primary and secondary hemorrhage among these surgical techniques, with a focus on guiding clinical decision-making. <b>Methodology</b>: A total of 12 studies, published between 2005 and 2024, were selected from the PubMed, Web of Science, Scopus, and Cochrane Library databases, comprising 1684 participants from both pediatric and adult groups. Primary and secondary hemorrhage rates, surgical techniques, and study characteristics were extracted as data. Therefore, the aim of performing this meta-analysis with random-effects models was to calculate pooled estimates for hemorrhage rates and the heterogeneity index (I<sup>2</sup>). The techniques studied included cold steel dissection, coblation, monopolar diathermy, and bipolar diathermy. <b>Results</b>: The pooled primary hemorrhage rate across all techniques was 1.0% (95% Cl: 0.5-1.4%), with insignificant heterogeneity (I<sup>2</sup> = 0.0%, <i>p</i> < 0.665). By contrast, pooled secondary hemorrhage occurred at a rate of 5.8% (95% CI: 3.9-7.6%). Cold steel tonsillectomy was associated with the lowest secondary hemorrhage rate of 3.7% (95% CI: 0.8-6.6%, I<sup>2</sup> = 43.558%, <i>p</i> = 0.115), while bipolar diathermy had the highest secondary hemorrhage rate of 8.6% (95% CI: 2.3-15.0%, I<sup>2</sup> = 86.448%, <i>p</i> < 0.001). <b>Conclusions</b>: This meta-analysis underscores the considerable variability in rates of post-tonsillectomy hemorrhage frequency among various surgical techniques. Cold steel dissection appears to be the safest regarding secondary hemorrhage, while coblation likely minimizes primary bleeding. Bipolar diathermy comes across as the technique with the highest risk for primary hemorrhage and requires special caution during its use. Such results emphasize the need for careful selection of the surgical technique concerning patients' particular conditions and the need to enhance care periods to reduce the bearing of any hemorrhagic complications.</p>","PeriodicalId":45306,"journal":{"name":"Clinics and Practice","volume":"15 5","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12110027/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of Post-Tonsillectomy Hemorrhage Rate After Different Tonsillectomy Techniques: Systematic Review and Meta Analysis.\",\"authors\":\"Mazyad M Alenezi, Faisal A Al-Harbi, Albaraa Nasser M Almoshigeh, Sultan S Alruqaie, Nada M Alshahrani, Alwaleed Mohammed Alamro, Abdulmalik Abdulaziz Aljulajil, Rayan Abduallah Alsaqri, Lama A Alharbi\",\"doi\":\"10.3390/clinpract15050085\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction</b>: Post-tonsillectomy hemorrhage is a serious complication that varies according to the surgical technique used, potentially compromising patient safety and recovery. Even though several techniques were frequently used, including cold steel dissection, coblation, monopolar diathermy, and bipolar diathermy, there were certain discrepancies in hemorrhage rates in the literature. This meta-analysis aims to compare the rates of primary and secondary hemorrhage among these surgical techniques, with a focus on guiding clinical decision-making. <b>Methodology</b>: A total of 12 studies, published between 2005 and 2024, were selected from the PubMed, Web of Science, Scopus, and Cochrane Library databases, comprising 1684 participants from both pediatric and adult groups. Primary and secondary hemorrhage rates, surgical techniques, and study characteristics were extracted as data. Therefore, the aim of performing this meta-analysis with random-effects models was to calculate pooled estimates for hemorrhage rates and the heterogeneity index (I<sup>2</sup>). The techniques studied included cold steel dissection, coblation, monopolar diathermy, and bipolar diathermy. <b>Results</b>: The pooled primary hemorrhage rate across all techniques was 1.0% (95% Cl: 0.5-1.4%), with insignificant heterogeneity (I<sup>2</sup> = 0.0%, <i>p</i> < 0.665). By contrast, pooled secondary hemorrhage occurred at a rate of 5.8% (95% CI: 3.9-7.6%). Cold steel tonsillectomy was associated with the lowest secondary hemorrhage rate of 3.7% (95% CI: 0.8-6.6%, I<sup>2</sup> = 43.558%, <i>p</i> = 0.115), while bipolar diathermy had the highest secondary hemorrhage rate of 8.6% (95% CI: 2.3-15.0%, I<sup>2</sup> = 86.448%, <i>p</i> < 0.001). <b>Conclusions</b>: This meta-analysis underscores the considerable variability in rates of post-tonsillectomy hemorrhage frequency among various surgical techniques. Cold steel dissection appears to be the safest regarding secondary hemorrhage, while coblation likely minimizes primary bleeding. Bipolar diathermy comes across as the technique with the highest risk for primary hemorrhage and requires special caution during its use. Such results emphasize the need for careful selection of the surgical technique concerning patients' particular conditions and the need to enhance care periods to reduce the bearing of any hemorrhagic complications.</p>\",\"PeriodicalId\":45306,\"journal\":{\"name\":\"Clinics and Practice\",\"volume\":\"15 5\",\"pages\":\"\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12110027/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinics and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/clinpract15050085\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/clinpract15050085","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
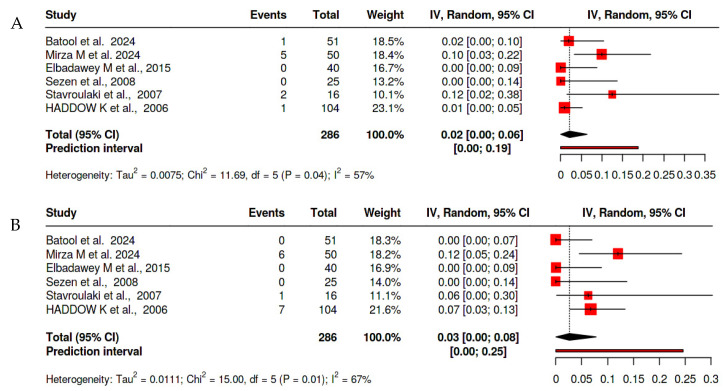
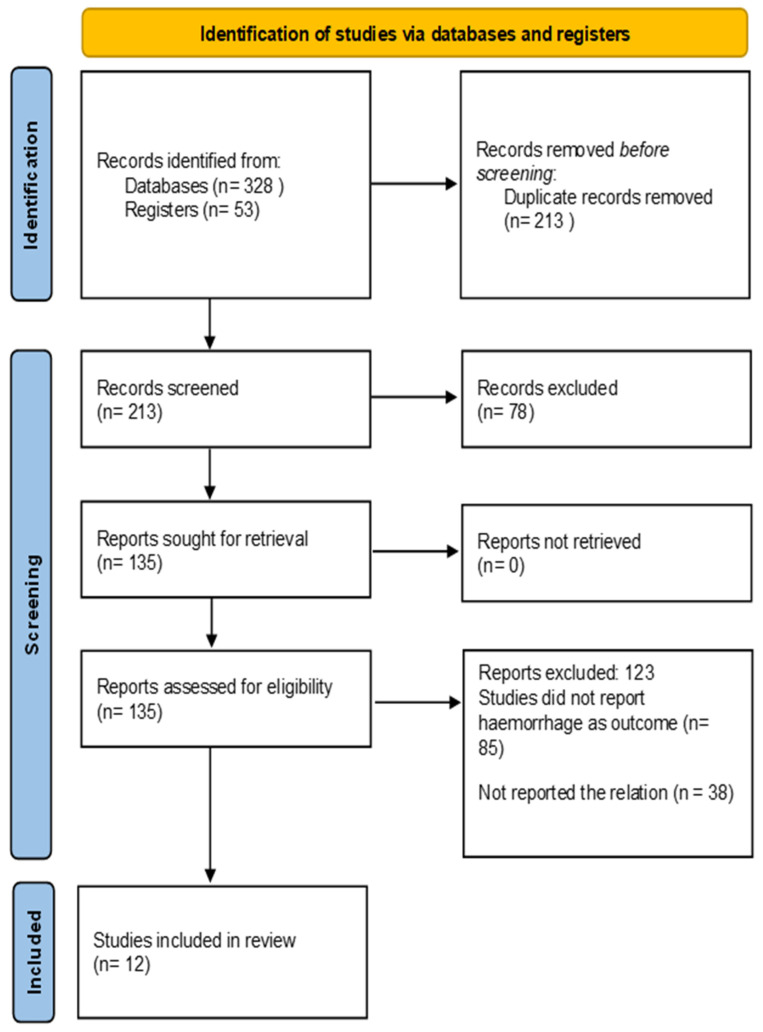
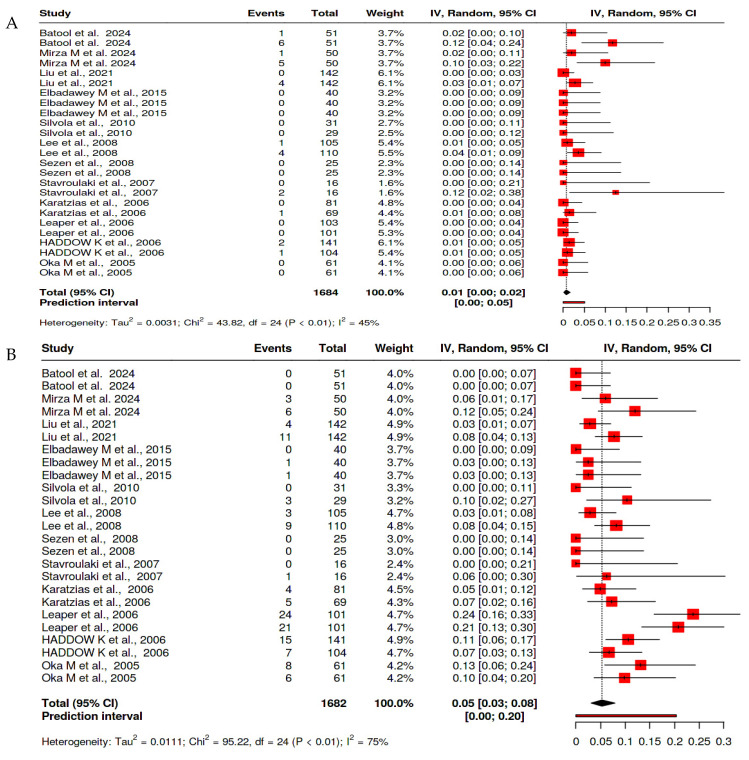
扁桃体切除术后出血是一种严重的并发症,根据手术技术的不同而不同,可能危及患者的安全和康复。尽管经常使用几种技术,包括冷钢解剖、消融、单极透热和双极透热,但在文献中出血率存在一定的差异。本荟萃分析旨在比较这些手术技术中原发性和继发性出血的发生率,重点是指导临床决策。方法:从PubMed、Web of Science、Scopus和Cochrane图书馆数据库中选择了2005年至2024年间发表的12项研究,包括来自儿科和成人群体的1684名参与者。提取原发性和继发性出血率、手术技术和研究特征作为数据。因此,使用随机效应模型进行meta分析的目的是计算出血率和异质性指数的汇总估计值(I2)。研究的技术包括冷钢解剖、凝固、单极透热和双极透热。结果:所有技术的合并原发性出血率为1.0% (95% Cl: 0.5-1.4%),异质性不显著(I2 = 0.0%, p < 0.665)。相比之下,继发性合并出血发生率为5.8% (95% CI: 3.9-7.6%)。冷钢扁桃体切除术继发出血发生率最低,为3.7% (95% CI: 0.8 ~ 6.6%, I2 = 43.558%, p = 0.115),双极热疗继发出血发生率最高,为8.6% (95% CI: 2.3 ~ 15.0%, I2 = 86.448%, p < 0.001)。结论:本荟萃分析强调了扁桃体切除术后出血频率在各种手术技术中的相当大的变异性。对于继发性出血,冷钢解剖似乎是最安全的,而消融可能最大限度地减少原发性出血。双极透热疗法被认为是原发性出血风险最高的技术,在使用过程中需要特别小心。这些结果强调需要根据患者的特殊情况仔细选择手术技术,并需要延长护理期以减少出血并发症的发生。
Comparison of Post-Tonsillectomy Hemorrhage Rate After Different Tonsillectomy Techniques: Systematic Review and Meta Analysis.
Introduction: Post-tonsillectomy hemorrhage is a serious complication that varies according to the surgical technique used, potentially compromising patient safety and recovery. Even though several techniques were frequently used, including cold steel dissection, coblation, monopolar diathermy, and bipolar diathermy, there were certain discrepancies in hemorrhage rates in the literature. This meta-analysis aims to compare the rates of primary and secondary hemorrhage among these surgical techniques, with a focus on guiding clinical decision-making. Methodology: A total of 12 studies, published between 2005 and 2024, were selected from the PubMed, Web of Science, Scopus, and Cochrane Library databases, comprising 1684 participants from both pediatric and adult groups. Primary and secondary hemorrhage rates, surgical techniques, and study characteristics were extracted as data. Therefore, the aim of performing this meta-analysis with random-effects models was to calculate pooled estimates for hemorrhage rates and the heterogeneity index (I2). The techniques studied included cold steel dissection, coblation, monopolar diathermy, and bipolar diathermy. Results: The pooled primary hemorrhage rate across all techniques was 1.0% (95% Cl: 0.5-1.4%), with insignificant heterogeneity (I2 = 0.0%, p < 0.665). By contrast, pooled secondary hemorrhage occurred at a rate of 5.8% (95% CI: 3.9-7.6%). Cold steel tonsillectomy was associated with the lowest secondary hemorrhage rate of 3.7% (95% CI: 0.8-6.6%, I2 = 43.558%, p = 0.115), while bipolar diathermy had the highest secondary hemorrhage rate of 8.6% (95% CI: 2.3-15.0%, I2 = 86.448%, p < 0.001). Conclusions: This meta-analysis underscores the considerable variability in rates of post-tonsillectomy hemorrhage frequency among various surgical techniques. Cold steel dissection appears to be the safest regarding secondary hemorrhage, while coblation likely minimizes primary bleeding. Bipolar diathermy comes across as the technique with the highest risk for primary hemorrhage and requires special caution during its use. Such results emphasize the need for careful selection of the surgical technique concerning patients' particular conditions and the need to enhance care periods to reduce the bearing of any hemorrhagic complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


