Shannon Dorsey, Rashed AlRasheed, Suzanne Eu Kerns, Rosemary D Meza, Noah Triplett, Esther Deblinger, Nathaniel Jungbluth, Lucy Berliner, Lavangi Naithani, Michael D Pullmann
{"title":"社区心理健康监督策略的随机对照试验研究。","authors":"Shannon Dorsey, Rashed AlRasheed, Suzanne Eu Kerns, Rosemary D Meza, Noah Triplett, Esther Deblinger, Nathaniel Jungbluth, Lucy Berliner, Lavangi Naithani, Michael D Pullmann","doi":"10.1177/26334895251330523","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Clinicians need supports beyond training to deliver evidence-based treatments with fidelity. Workplace-based clinical supervision often is a commonly provided support in community mental health, yet too few studies have empirically examined supervision and its impact on clinician fidelity and treatment delivery.</p><p><strong>Method: </strong>Building on a Washington State-funded evidence-based treatment initiative (CBT+), we conducted a randomized controlled trial (RCT), testing two supervision conditions delivered by workplace-based supervisors (supervisors employed by community mental health organizations). The RCT followed a supervision-as-usual (SAU) phase for comparison. The treatment of focus was trauma-focused cognitive behavioral therapy (TF-CBT). Clinicians (<i>N</i> = 238) from 25 organizations participated in the study across the SAU baseline and RCT phases. In the RCT phase, clinicians were randomized to either symptom and fidelity monitoring (SFM) or SFM and behavioral rehearsal (SFM + BR). For BR, clinicians engaged in a short role play of an upcoming treatment element. Supervisors delivered both conditions, with regular study monitoring for drift. Clinicians audiorecorded therapy sessions with enrolled clients, and masked coders coded a subset of recordings for adherence to TF-CBT. One hundred and thirty-three clinicians had recorded TF-CBT session data for 258 youth. We examined six adherence outcomes, including potential moderators.</p><p><strong>Results: </strong>Results of generalized estimating equations indicated that there were no real differences on adherence outcomes for experimental conditions (SFM, SFM + BR) compared to SAU. Adherence scores in the baseline SAU phase and the RCT conditions were high. Only one interaction was significant.</p><p><strong>Conclusions: </strong>Contrary to our hypotheses, we did not see improvements in adherence with the RCT conditions. However, nonsignificant findings seem best explained by clinicians' acceptable/high adherence in SAU. This study was conducted within the context of a long-standing, state-funded EBT initiative, in which clinicians and their supervisors receive training and support, and in which participating community mental health organizations have adopted and supported TF-CBT.</p><p><strong>Clinicaltrialsgov id: </strong>NCT01800266.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"6 ","pages":"26334895251330523"},"PeriodicalIF":2.6000,"publicationDate":"2025-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12102572/pdf/","citationCount":"0","resultStr":"{\"title\":\"A randomized controlled trial testing supervision strategies in community mental health.\",\"authors\":\"Shannon Dorsey, Rashed AlRasheed, Suzanne Eu Kerns, Rosemary D Meza, Noah Triplett, Esther Deblinger, Nathaniel Jungbluth, Lucy Berliner, Lavangi Naithani, Michael D Pullmann\",\"doi\":\"10.1177/26334895251330523\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Clinicians need supports beyond training to deliver evidence-based treatments with fidelity. Workplace-based clinical supervision often is a commonly provided support in community mental health, yet too few studies have empirically examined supervision and its impact on clinician fidelity and treatment delivery.</p><p><strong>Method: </strong>Building on a Washington State-funded evidence-based treatment initiative (CBT+), we conducted a randomized controlled trial (RCT), testing two supervision conditions delivered by workplace-based supervisors (supervisors employed by community mental health organizations). The RCT followed a supervision-as-usual (SAU) phase for comparison. The treatment of focus was trauma-focused cognitive behavioral therapy (TF-CBT). Clinicians (<i>N</i> = 238) from 25 organizations participated in the study across the SAU baseline and RCT phases. In the RCT phase, clinicians were randomized to either symptom and fidelity monitoring (SFM) or SFM and behavioral rehearsal (SFM + BR). For BR, clinicians engaged in a short role play of an upcoming treatment element. Supervisors delivered both conditions, with regular study monitoring for drift. Clinicians audiorecorded therapy sessions with enrolled clients, and masked coders coded a subset of recordings for adherence to TF-CBT. One hundred and thirty-three clinicians had recorded TF-CBT session data for 258 youth. We examined six adherence outcomes, including potential moderators.</p><p><strong>Results: </strong>Results of generalized estimating equations indicated that there were no real differences on adherence outcomes for experimental conditions (SFM, SFM + BR) compared to SAU. Adherence scores in the baseline SAU phase and the RCT conditions were high. Only one interaction was significant.</p><p><strong>Conclusions: </strong>Contrary to our hypotheses, we did not see improvements in adherence with the RCT conditions. However, nonsignificant findings seem best explained by clinicians' acceptable/high adherence in SAU. This study was conducted within the context of a long-standing, state-funded EBT initiative, in which clinicians and their supervisors receive training and support, and in which participating community mental health organizations have adopted and supported TF-CBT.</p><p><strong>Clinicaltrialsgov id: </strong>NCT01800266.</p>\",\"PeriodicalId\":73354,\"journal\":{\"name\":\"Implementation research and practice\",\"volume\":\"6 \",\"pages\":\"26334895251330523\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12102572/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Implementation research and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/26334895251330523\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895251330523","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A randomized controlled trial testing supervision strategies in community mental health.
Background: Clinicians need supports beyond training to deliver evidence-based treatments with fidelity. Workplace-based clinical supervision often is a commonly provided support in community mental health, yet too few studies have empirically examined supervision and its impact on clinician fidelity and treatment delivery.
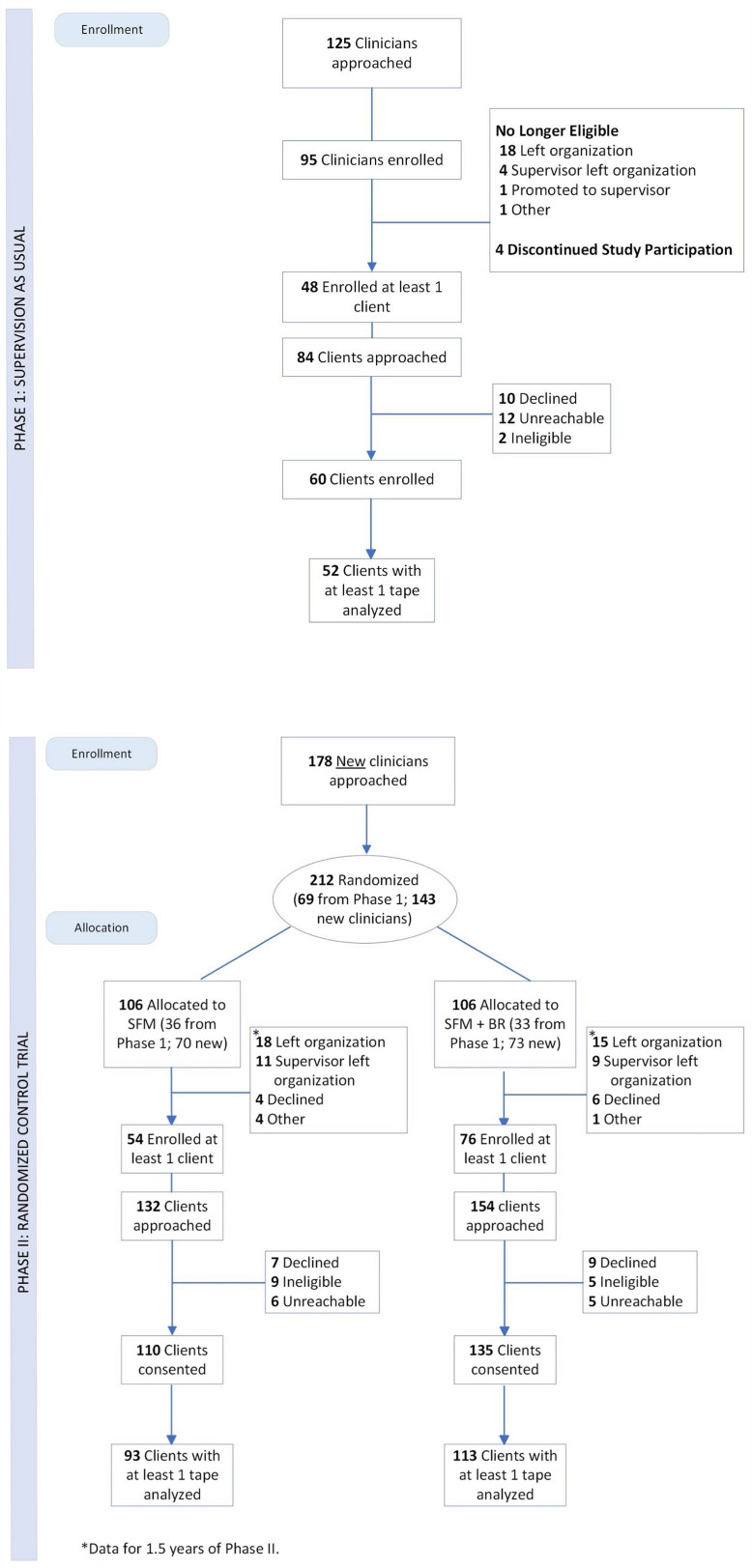
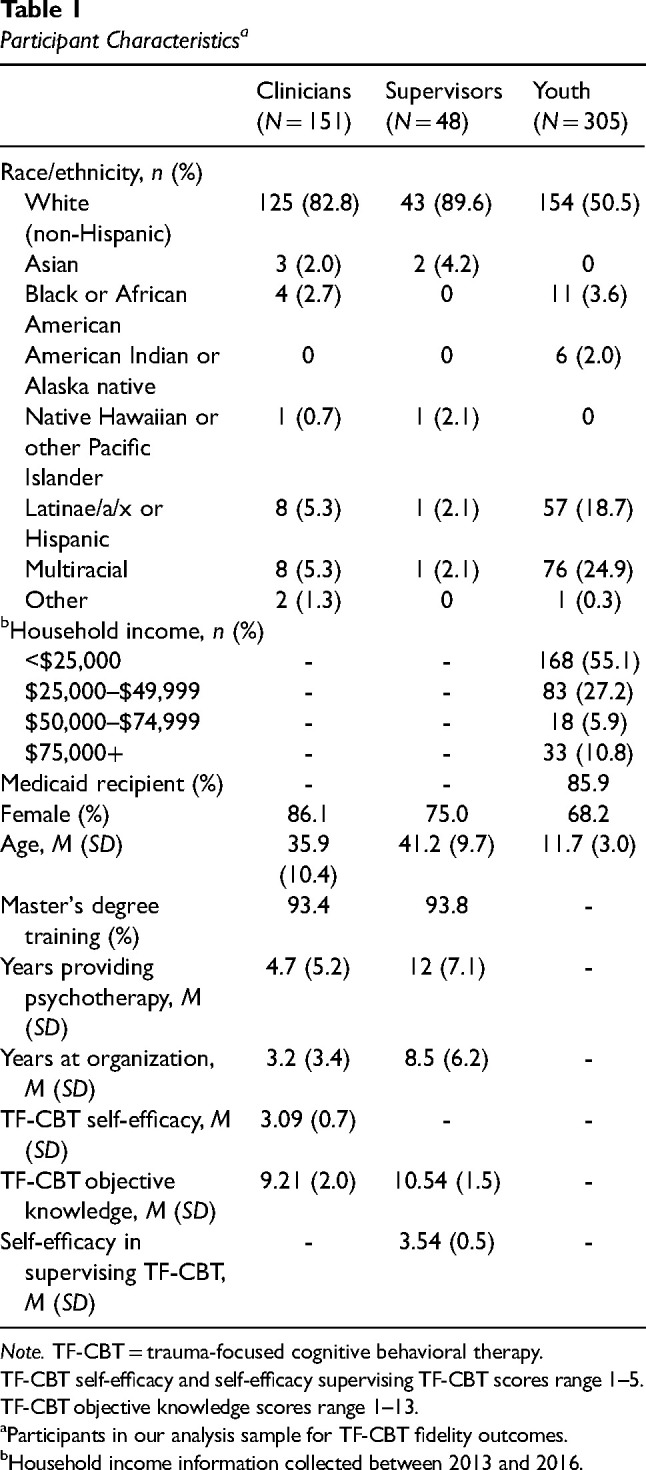
Method: Building on a Washington State-funded evidence-based treatment initiative (CBT+), we conducted a randomized controlled trial (RCT), testing two supervision conditions delivered by workplace-based supervisors (supervisors employed by community mental health organizations). The RCT followed a supervision-as-usual (SAU) phase for comparison. The treatment of focus was trauma-focused cognitive behavioral therapy (TF-CBT). Clinicians (N = 238) from 25 organizations participated in the study across the SAU baseline and RCT phases. In the RCT phase, clinicians were randomized to either symptom and fidelity monitoring (SFM) or SFM and behavioral rehearsal (SFM + BR). For BR, clinicians engaged in a short role play of an upcoming treatment element. Supervisors delivered both conditions, with regular study monitoring for drift. Clinicians audiorecorded therapy sessions with enrolled clients, and masked coders coded a subset of recordings for adherence to TF-CBT. One hundred and thirty-three clinicians had recorded TF-CBT session data for 258 youth. We examined six adherence outcomes, including potential moderators.
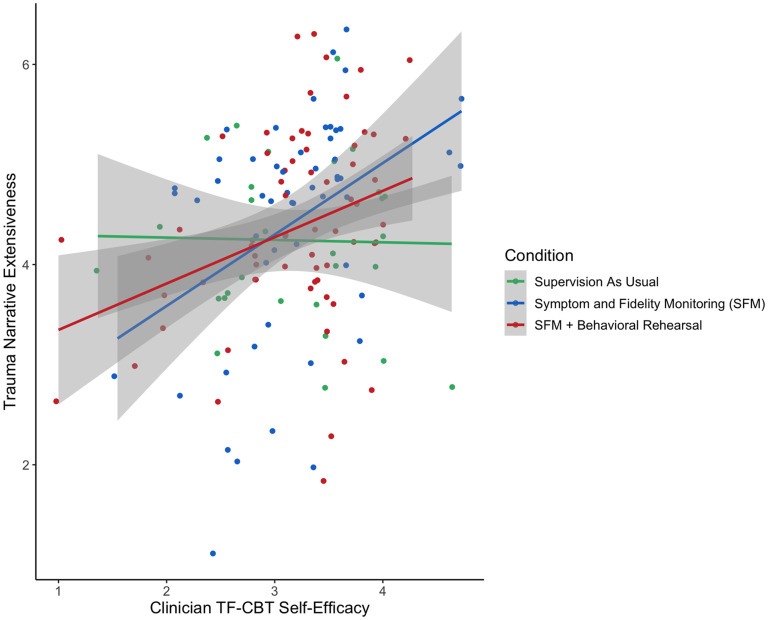
Results: Results of generalized estimating equations indicated that there were no real differences on adherence outcomes for experimental conditions (SFM, SFM + BR) compared to SAU. Adherence scores in the baseline SAU phase and the RCT conditions were high. Only one interaction was significant.
Conclusions: Contrary to our hypotheses, we did not see improvements in adherence with the RCT conditions. However, nonsignificant findings seem best explained by clinicians' acceptable/high adherence in SAU. This study was conducted within the context of a long-standing, state-funded EBT initiative, in which clinicians and their supervisors receive training and support, and in which participating community mental health organizations have adopted and supported TF-CBT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


