Ahmet Tas, Yaren Alan, Ilke Kara Tas, Sabahattin Umman, Kim H Parker, Tim P van de Hoef, Murat Sezer, Jan J Piek
{"title":"高微血管阻力对冠状动脉波能量的影响取决于冠状动脉微血管功能。","authors":"Ahmet Tas, Yaren Alan, Ilke Kara Tas, Sabahattin Umman, Kim H Parker, Tim P van de Hoef, Murat Sezer, Jan J Piek","doi":"10.1093/ehjopen/oeaf050","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The pathophysiological relevance of high hyperemic microvascular resistance (hMR) in stable coronary artery disease is controversial. Using wave intensity analysis (WIA, defined as the product of the time derivatives of the coronary pressure and velocity), we aim to compare the impact of high hMR on coronary wave energetics with respect to coronary microvascular dysfunction (CMD), defined as reduced coronary flow reserve (CFR < 2.5), in unobstructed arteries.</p><p><strong>Methods and results: </strong>The study population (<i>n</i> = 258, mean age = 68 ± 10 years, 73% male) had a high cardiovascular risk profile including dyslipidemia (88%), hypertension (70%), smoking (55%) and diabetes (28%). The mean fractional flow reserve was 0.89 ± 0.05. Vessels (<i>n</i> = 312) were divided into four endotypes: no CMD-low hMR (CFR ≥ 2.5, hMR < 2.5 mmHg.s.cm<sup>-1</sup>), Functional CMD (CFR < 2.5, hMR < 2.5 mmHg.s.cm<sup>-1</sup>), Structural CMD (CFR < 2.5, hMR ≥ 2.5 mmHg.s.cm<sup>-1</sup>), and no CMD-high hMR (CFR ≥ 2.5, hMR ≥ 2.5 mmHg.s.cm<sup>-1</sup>). The no CMD-high hMR endotype had the lowest mean resting velocity (bAPV = 10 ± 3 cm.s<sup>-1</sup> <i>P</i> < 0.001), highest mean basal microvascular resistance (bMR = 9 ± 2 mmHg/cm.s<sup>-1</sup> <i>P</i> < 0.001) amongst all endotypes, yet, it had reference-level CFR, microvascular resistance reserve and resistive reserve ratio (<i>P</i> > 0.05 for all compared to no CMD-low hMR), unlike CMD endotypes (<i>P</i> < 0.05 compared to CMD endotypes). The no CMD-high hMR endotype exhibited the highest hyperemic increase in the accelerating wave energy proportion (AEP) (13% ± 13%, <i>P</i> = 0.042), indicating an intact autoregulatory response. Only in the CMD endotypes, high hMR was associated with reduced AEP (<i>r</i> = -0.229, <i>P</i> < 0.001), unlike no CMD endotypes (<i>P</i> = 0.383).</p><p><strong>Conclusion: </strong>High hMR alone is not a definitive CMD marker. In line with the adaptive high hMR hypothesis, increased hMR does not necessarily limit augmentation of AEP, and is associated with robust autoregulatory capacity in vessels with preserved CFR. Cardiologists should be alert to a potential adaptive no CMD-high hMR endotype to avoid misdiagnosis.</p><p><strong>Registration: </strong>NCT02328820.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf050"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12100483/pdf/","citationCount":"0","resultStr":"{\"title\":\"The impact of high microvascular resistance on coronary wave energetics depends on coronary microvascular functionality.\",\"authors\":\"Ahmet Tas, Yaren Alan, Ilke Kara Tas, Sabahattin Umman, Kim H Parker, Tim P van de Hoef, Murat Sezer, Jan J Piek\",\"doi\":\"10.1093/ehjopen/oeaf050\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The pathophysiological relevance of high hyperemic microvascular resistance (hMR) in stable coronary artery disease is controversial. Using wave intensity analysis (WIA, defined as the product of the time derivatives of the coronary pressure and velocity), we aim to compare the impact of high hMR on coronary wave energetics with respect to coronary microvascular dysfunction (CMD), defined as reduced coronary flow reserve (CFR < 2.5), in unobstructed arteries.</p><p><strong>Methods and results: </strong>The study population (<i>n</i> = 258, mean age = 68 ± 10 years, 73% male) had a high cardiovascular risk profile including dyslipidemia (88%), hypertension (70%), smoking (55%) and diabetes (28%). The mean fractional flow reserve was 0.89 ± 0.05. Vessels (<i>n</i> = 312) were divided into four endotypes: no CMD-low hMR (CFR ≥ 2.5, hMR < 2.5 mmHg.s.cm<sup>-1</sup>), Functional CMD (CFR < 2.5, hMR < 2.5 mmHg.s.cm<sup>-1</sup>), Structural CMD (CFR < 2.5, hMR ≥ 2.5 mmHg.s.cm<sup>-1</sup>), and no CMD-high hMR (CFR ≥ 2.5, hMR ≥ 2.5 mmHg.s.cm<sup>-1</sup>). The no CMD-high hMR endotype had the lowest mean resting velocity (bAPV = 10 ± 3 cm.s<sup>-1</sup> <i>P</i> < 0.001), highest mean basal microvascular resistance (bMR = 9 ± 2 mmHg/cm.s<sup>-1</sup> <i>P</i> < 0.001) amongst all endotypes, yet, it had reference-level CFR, microvascular resistance reserve and resistive reserve ratio (<i>P</i> > 0.05 for all compared to no CMD-low hMR), unlike CMD endotypes (<i>P</i> < 0.05 compared to CMD endotypes). The no CMD-high hMR endotype exhibited the highest hyperemic increase in the accelerating wave energy proportion (AEP) (13% ± 13%, <i>P</i> = 0.042), indicating an intact autoregulatory response. Only in the CMD endotypes, high hMR was associated with reduced AEP (<i>r</i> = -0.229, <i>P</i> < 0.001), unlike no CMD endotypes (<i>P</i> = 0.383).</p><p><strong>Conclusion: </strong>High hMR alone is not a definitive CMD marker. In line with the adaptive high hMR hypothesis, increased hMR does not necessarily limit augmentation of AEP, and is associated with robust autoregulatory capacity in vessels with preserved CFR. Cardiologists should be alert to a potential adaptive no CMD-high hMR endotype to avoid misdiagnosis.</p><p><strong>Registration: </strong>NCT02328820.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 3\",\"pages\":\"oeaf050\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-05-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12100483/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf050\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf050","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
The impact of high microvascular resistance on coronary wave energetics depends on coronary microvascular functionality.
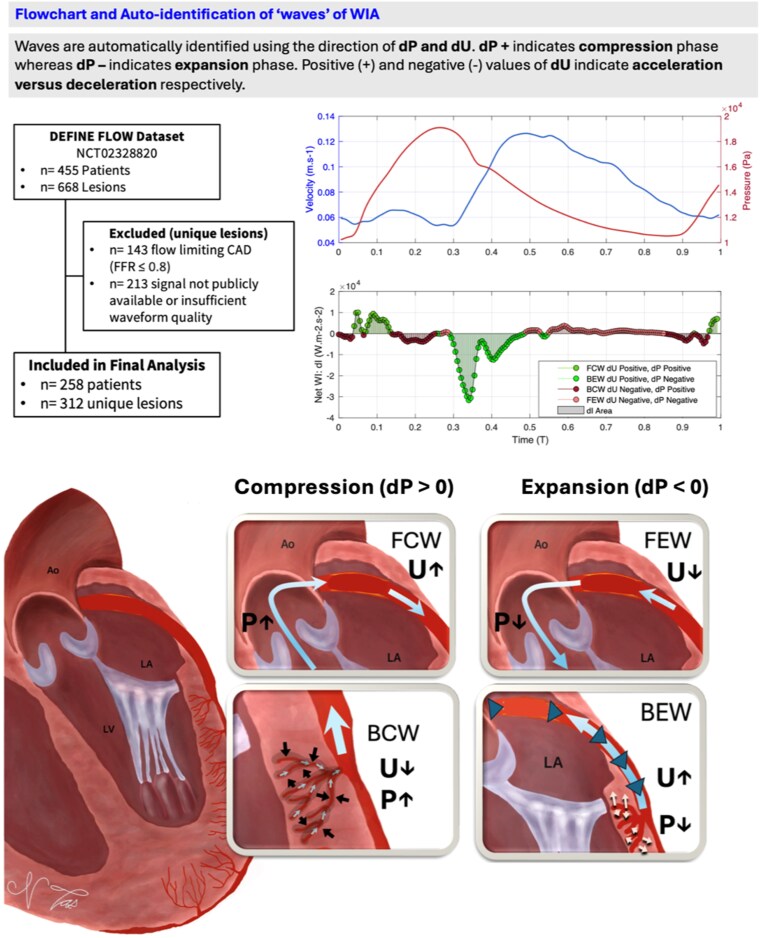
Aims: The pathophysiological relevance of high hyperemic microvascular resistance (hMR) in stable coronary artery disease is controversial. Using wave intensity analysis (WIA, defined as the product of the time derivatives of the coronary pressure and velocity), we aim to compare the impact of high hMR on coronary wave energetics with respect to coronary microvascular dysfunction (CMD), defined as reduced coronary flow reserve (CFR < 2.5), in unobstructed arteries.
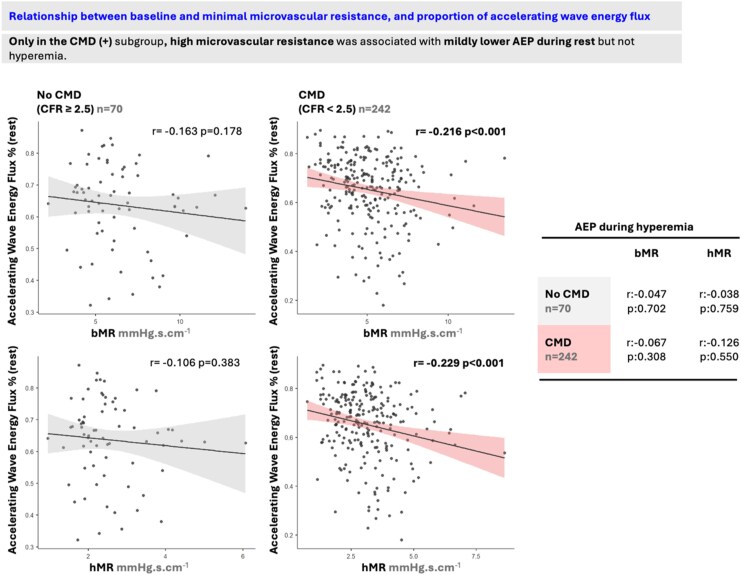
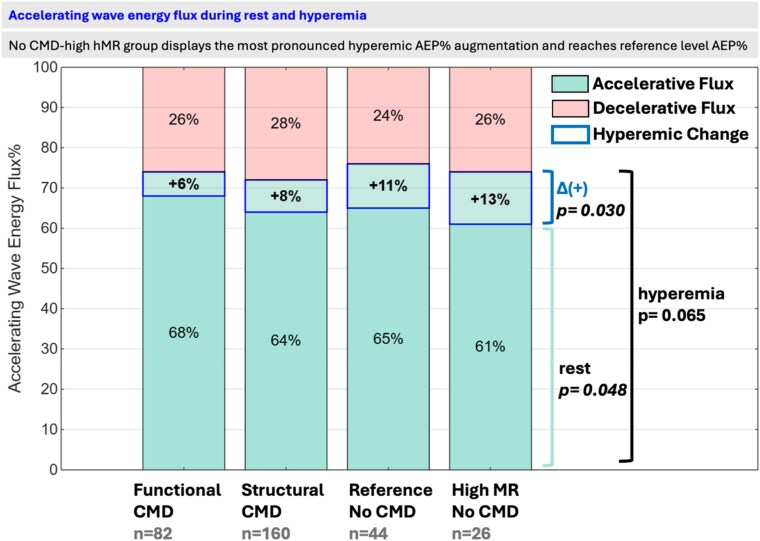
Methods and results: The study population (n = 258, mean age = 68 ± 10 years, 73% male) had a high cardiovascular risk profile including dyslipidemia (88%), hypertension (70%), smoking (55%) and diabetes (28%). The mean fractional flow reserve was 0.89 ± 0.05. Vessels (n = 312) were divided into four endotypes: no CMD-low hMR (CFR ≥ 2.5, hMR < 2.5 mmHg.s.cm-1), Functional CMD (CFR < 2.5, hMR < 2.5 mmHg.s.cm-1), Structural CMD (CFR < 2.5, hMR ≥ 2.5 mmHg.s.cm-1), and no CMD-high hMR (CFR ≥ 2.5, hMR ≥ 2.5 mmHg.s.cm-1). The no CMD-high hMR endotype had the lowest mean resting velocity (bAPV = 10 ± 3 cm.s-1P < 0.001), highest mean basal microvascular resistance (bMR = 9 ± 2 mmHg/cm.s-1P < 0.001) amongst all endotypes, yet, it had reference-level CFR, microvascular resistance reserve and resistive reserve ratio (P > 0.05 for all compared to no CMD-low hMR), unlike CMD endotypes (P < 0.05 compared to CMD endotypes). The no CMD-high hMR endotype exhibited the highest hyperemic increase in the accelerating wave energy proportion (AEP) (13% ± 13%, P = 0.042), indicating an intact autoregulatory response. Only in the CMD endotypes, high hMR was associated with reduced AEP (r = -0.229, P < 0.001), unlike no CMD endotypes (P = 0.383).
Conclusion: High hMR alone is not a definitive CMD marker. In line with the adaptive high hMR hypothesis, increased hMR does not necessarily limit augmentation of AEP, and is associated with robust autoregulatory capacity in vessels with preserved CFR. Cardiologists should be alert to a potential adaptive no CMD-high hMR endotype to avoid misdiagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


