Ian M McElree, Ryan L Steinberg, Sarah L Mott, Helen Y Hougen, Michael A O'Donnell, Vignesh T Packiam
{"title":"在高危NMIBC诱导治疗后的首次监测中,蓝光膀胱镜检查和其他手术评估的作用。","authors":"Ian M McElree, Ryan L Steinberg, Sarah L Mott, Helen Y Hougen, Michael A O'Donnell, Vignesh T Packiam","doi":"10.1177/23523735251324318","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>During surveillance of high-risk non-muscle invasive bladder cancer (HR-NMIBC), occult disease can be missed by standard cystoscopy.</p><p><strong>Objective: </strong>To determine the utility of enhanced restaging procedures.</p><p><strong>Methods: </strong>We retrospectively reviewed 297 patients with HR-NMIBC who underwent enhanced restaging procedures during the first surveillance following induction intravesical therapy between 2010-2021. Patients were stratified by number of induction treatments with unique agents (161, 63, and 73 patients with 1, 2, and 3+ treatments) and analyzed using exact logistic regression models. Enhanced restaging procedures included standard cystoscopy (white-light cystoscopy with bladder wash cytology) plus additional components including blue-light cystoscopy, mapping bladder biopsies, retrograde pyelograms, upper tract cytologies, and prostatic urethral biopsies.</p><p><strong>Results: </strong>When standard cystoscopy was negative, blue light cystoscopy detected occult bladder cancer in 6.0%, 7.4%, and 19% of patients in the 1, 2, and 3+ treatment groups. History of CIS was associated with increased detection with blue light (p = 0.03). Extravesical (upper tract or prostatic urethral) cancer was detected by additional restaging components in 0.6%, 1.7%, and 15% of patients with 1, 2, and 3+ intravesical treatments. On multivariable analysis, receipt of 3+ intravesical inductions increased the odds of having at least one additional restaging component identify cancer (HR 3.76; p < .01).</p><p><strong>Conclusions: </strong>Blue light cystoscopy improves surveillance of HR-NMIBC, particularly in those with CIS. Additional restaging procedures improved detection of extravesical disease in patients with heavier pre-treatment history. Risk-adapted utilization of enhanced restaging procedures requires further study.</p>","PeriodicalId":54217,"journal":{"name":"Bladder Cancer","volume":"11 2","pages":"23523735251324318"},"PeriodicalIF":1.2000,"publicationDate":"2025-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12102550/pdf/","citationCount":"0","resultStr":"{\"title\":\"The role of blue light cystoscopy and additional operative evaluations during first surveillance after induction therapy for high-risk NMIBC.\",\"authors\":\"Ian M McElree, Ryan L Steinberg, Sarah L Mott, Helen Y Hougen, Michael A O'Donnell, Vignesh T Packiam\",\"doi\":\"10.1177/23523735251324318\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>During surveillance of high-risk non-muscle invasive bladder cancer (HR-NMIBC), occult disease can be missed by standard cystoscopy.</p><p><strong>Objective: </strong>To determine the utility of enhanced restaging procedures.</p><p><strong>Methods: </strong>We retrospectively reviewed 297 patients with HR-NMIBC who underwent enhanced restaging procedures during the first surveillance following induction intravesical therapy between 2010-2021. Patients were stratified by number of induction treatments with unique agents (161, 63, and 73 patients with 1, 2, and 3+ treatments) and analyzed using exact logistic regression models. Enhanced restaging procedures included standard cystoscopy (white-light cystoscopy with bladder wash cytology) plus additional components including blue-light cystoscopy, mapping bladder biopsies, retrograde pyelograms, upper tract cytologies, and prostatic urethral biopsies.</p><p><strong>Results: </strong>When standard cystoscopy was negative, blue light cystoscopy detected occult bladder cancer in 6.0%, 7.4%, and 19% of patients in the 1, 2, and 3+ treatment groups. History of CIS was associated with increased detection with blue light (p = 0.03). Extravesical (upper tract or prostatic urethral) cancer was detected by additional restaging components in 0.6%, 1.7%, and 15% of patients with 1, 2, and 3+ intravesical treatments. On multivariable analysis, receipt of 3+ intravesical inductions increased the odds of having at least one additional restaging component identify cancer (HR 3.76; p < .01).</p><p><strong>Conclusions: </strong>Blue light cystoscopy improves surveillance of HR-NMIBC, particularly in those with CIS. Additional restaging procedures improved detection of extravesical disease in patients with heavier pre-treatment history. Risk-adapted utilization of enhanced restaging procedures requires further study.</p>\",\"PeriodicalId\":54217,\"journal\":{\"name\":\"Bladder Cancer\",\"volume\":\"11 2\",\"pages\":\"23523735251324318\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2025-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12102550/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bladder Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/23523735251324318\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bladder Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/23523735251324318","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
The role of blue light cystoscopy and additional operative evaluations during first surveillance after induction therapy for high-risk NMIBC.
Background: During surveillance of high-risk non-muscle invasive bladder cancer (HR-NMIBC), occult disease can be missed by standard cystoscopy.
Objective: To determine the utility of enhanced restaging procedures.
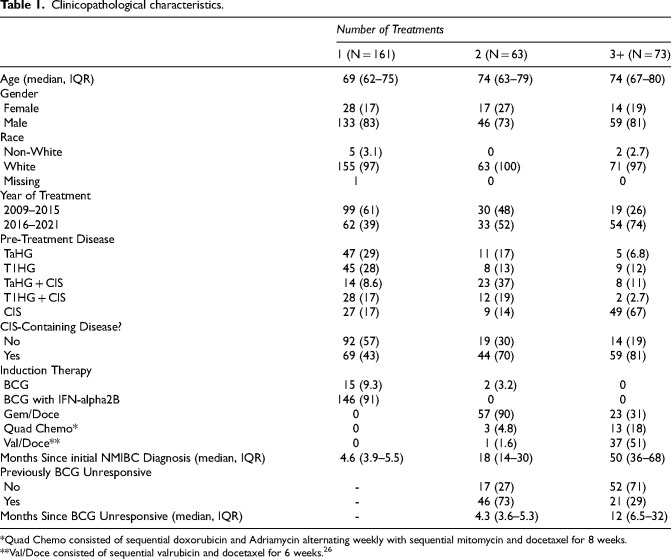
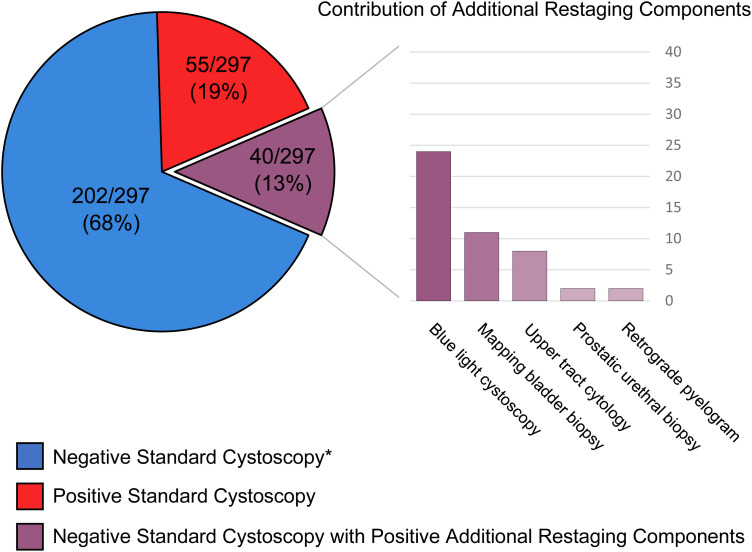
Methods: We retrospectively reviewed 297 patients with HR-NMIBC who underwent enhanced restaging procedures during the first surveillance following induction intravesical therapy between 2010-2021. Patients were stratified by number of induction treatments with unique agents (161, 63, and 73 patients with 1, 2, and 3+ treatments) and analyzed using exact logistic regression models. Enhanced restaging procedures included standard cystoscopy (white-light cystoscopy with bladder wash cytology) plus additional components including blue-light cystoscopy, mapping bladder biopsies, retrograde pyelograms, upper tract cytologies, and prostatic urethral biopsies.
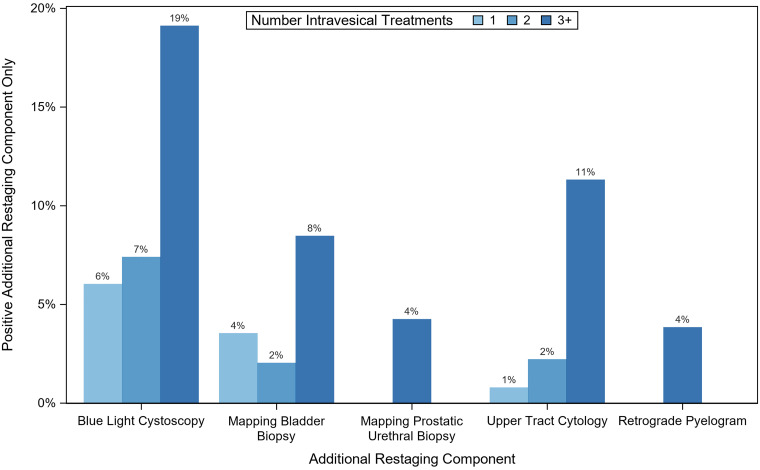
Results: When standard cystoscopy was negative, blue light cystoscopy detected occult bladder cancer in 6.0%, 7.4%, and 19% of patients in the 1, 2, and 3+ treatment groups. History of CIS was associated with increased detection with blue light (p = 0.03). Extravesical (upper tract or prostatic urethral) cancer was detected by additional restaging components in 0.6%, 1.7%, and 15% of patients with 1, 2, and 3+ intravesical treatments. On multivariable analysis, receipt of 3+ intravesical inductions increased the odds of having at least one additional restaging component identify cancer (HR 3.76; p < .01).
Conclusions: Blue light cystoscopy improves surveillance of HR-NMIBC, particularly in those with CIS. Additional restaging procedures improved detection of extravesical disease in patients with heavier pre-treatment history. Risk-adapted utilization of enhanced restaging procedures requires further study.
期刊介绍:
Bladder Cancer is an international multidisciplinary journal to facilitate progress in understanding the epidemiology/etiology, genetics, molecular correlates, pathogenesis, pharmacology, ethics, patient advocacy and survivorship, diagnosis and treatment of tumors of the bladder and upper urinary tract. The journal publishes research reports, reviews, short communications, and letters-to-the-editor. The journal is dedicated to providing an open forum for original research in basic science, translational research and clinical medicine that expedites our fundamental understanding and improves treatment of tumors of the bladder and upper urinary tract.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


