Jonathan B Bell, Sulaiman Sheriff, Mohammed Z Goryawala, Kaylie Cullison, Gregory A Azzam, Jessica Meshman, Matthew C Abramowitz, Michael E Ivan, Macarena I de la Fuente, Eric A Mellon
{"title":"用MRI光谱定义胶质母细胞瘤的隐匿性疾病:对临床靶体积描绘的意义。","authors":"Jonathan B Bell, Sulaiman Sheriff, Mohammed Z Goryawala, Kaylie Cullison, Gregory A Azzam, Jessica Meshman, Matthew C Abramowitz, Michael E Ivan, Macarena I de la Fuente, Eric A Mellon","doi":"10.1186/s13014-025-02666-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Outcomes in glioblastoma are improved by surgical resection and adjuvant radiation (RT). In primary GBM (pGBM), large clinical target volume (CTV) margins typically cover occult invasion. In recurrent GBM (rGBM), RT often uses tiny CTV margins that likely omit occult invasion due to re-RT radiation necrosis concerns. Whole-brain spectroscopic MRI (sMRI) is an emerging technique with similar resolution to PET that may help define the CTV for rGBM.</p><p><strong>Methods: </strong>Patients with pGBM (n = 18) and rGBM (n = 19) underwent sMRI with RT simulation. T1-post contrast (T1PC) and T2/FLAIR MRI volumes were contoured. sMRI generated choline/N-acetylaspartate > 2x (Cho/NAA > 2x) volumes are known to correlate with high-risk invasion. Hausdorff distances were calculated to define the margin necessary to cover Cho/NAA > 2x in pGBM and rGBM. In rGBM, mock CTV expansions from T1PC volumes were created to determine non-selective CTV expansion sizes needed to cover Cho/NAA > 2x volumes.</p><p><strong>Results: </strong>For pGBM, the median T1PC, Cho/NAA > 2x, and T2/FLAIR volumes were 32.3 cc, 45.0 cc, and 74.8 cc respectively. For rGBM, the median T1PC, Cho/NAA > 2x, and T2/FLAIR volumes were 21.7 cc, 58.9 cc, and 118.3 cc, respectively. T2/FLAIR volumes increased more relative to T1PC volumes in rGBM than pGBM (p ≤ 0.001). Meanwhile, the median Hausdorff distance between T1PC and Cho/NAA > 2x was 22.9 mm in pGBM and 25.7 mm in rGBM, suggesting that the high-risk volume does not significantly change. In rGBM, it is common to use no CTV expansion from the T1PC volume which only included 61% of high-risk Cho/NAA > 2x volume. Conversely, T1PC expansions of 10-, 15-, and 20-mm covered 87%, 94%, and 98% of Cho/NAA > 2x volume.</p><p><strong>Conclusions: </strong>sMRI Cho/NAA > 2x delineates high-risk occult disease in glioblastoma and extends beyond T1PC MRI borders. Typical large CTV expansions in pGBM mostly include Cho/NAA > 2x volumes. However, small CTV expansions commonly used in rGBM poorly cover Cho/NAA > 2x, suggesting that larger CTV expansions or Cho/NAA > 2x guidance may be of benefit.</p>","PeriodicalId":49639,"journal":{"name":"Radiation Oncology","volume":"20 1","pages":"86"},"PeriodicalIF":3.3000,"publicationDate":"2025-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12100854/pdf/","citationCount":"0","resultStr":"{\"title\":\"Defining occult disease in glioblastoma using spectroscopic MRI: implications for clinical target volume delineation.\",\"authors\":\"Jonathan B Bell, Sulaiman Sheriff, Mohammed Z Goryawala, Kaylie Cullison, Gregory A Azzam, Jessica Meshman, Matthew C Abramowitz, Michael E Ivan, Macarena I de la Fuente, Eric A Mellon\",\"doi\":\"10.1186/s13014-025-02666-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Outcomes in glioblastoma are improved by surgical resection and adjuvant radiation (RT). In primary GBM (pGBM), large clinical target volume (CTV) margins typically cover occult invasion. In recurrent GBM (rGBM), RT often uses tiny CTV margins that likely omit occult invasion due to re-RT radiation necrosis concerns. Whole-brain spectroscopic MRI (sMRI) is an emerging technique with similar resolution to PET that may help define the CTV for rGBM.</p><p><strong>Methods: </strong>Patients with pGBM (n = 18) and rGBM (n = 19) underwent sMRI with RT simulation. T1-post contrast (T1PC) and T2/FLAIR MRI volumes were contoured. sMRI generated choline/N-acetylaspartate > 2x (Cho/NAA > 2x) volumes are known to correlate with high-risk invasion. Hausdorff distances were calculated to define the margin necessary to cover Cho/NAA > 2x in pGBM and rGBM. In rGBM, mock CTV expansions from T1PC volumes were created to determine non-selective CTV expansion sizes needed to cover Cho/NAA > 2x volumes.</p><p><strong>Results: </strong>For pGBM, the median T1PC, Cho/NAA > 2x, and T2/FLAIR volumes were 32.3 cc, 45.0 cc, and 74.8 cc respectively. For rGBM, the median T1PC, Cho/NAA > 2x, and T2/FLAIR volumes were 21.7 cc, 58.9 cc, and 118.3 cc, respectively. T2/FLAIR volumes increased more relative to T1PC volumes in rGBM than pGBM (p ≤ 0.001). Meanwhile, the median Hausdorff distance between T1PC and Cho/NAA > 2x was 22.9 mm in pGBM and 25.7 mm in rGBM, suggesting that the high-risk volume does not significantly change. In rGBM, it is common to use no CTV expansion from the T1PC volume which only included 61% of high-risk Cho/NAA > 2x volume. Conversely, T1PC expansions of 10-, 15-, and 20-mm covered 87%, 94%, and 98% of Cho/NAA > 2x volume.</p><p><strong>Conclusions: </strong>sMRI Cho/NAA > 2x delineates high-risk occult disease in glioblastoma and extends beyond T1PC MRI borders. Typical large CTV expansions in pGBM mostly include Cho/NAA > 2x volumes. However, small CTV expansions commonly used in rGBM poorly cover Cho/NAA > 2x, suggesting that larger CTV expansions or Cho/NAA > 2x guidance may be of benefit.</p>\",\"PeriodicalId\":49639,\"journal\":{\"name\":\"Radiation Oncology\",\"volume\":\"20 1\",\"pages\":\"86\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2025-05-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12100854/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiation Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13014-025-02666-z\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13014-025-02666-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Defining occult disease in glioblastoma using spectroscopic MRI: implications for clinical target volume delineation.
Background: Outcomes in glioblastoma are improved by surgical resection and adjuvant radiation (RT). In primary GBM (pGBM), large clinical target volume (CTV) margins typically cover occult invasion. In recurrent GBM (rGBM), RT often uses tiny CTV margins that likely omit occult invasion due to re-RT radiation necrosis concerns. Whole-brain spectroscopic MRI (sMRI) is an emerging technique with similar resolution to PET that may help define the CTV for rGBM.
Methods: Patients with pGBM (n = 18) and rGBM (n = 19) underwent sMRI with RT simulation. T1-post contrast (T1PC) and T2/FLAIR MRI volumes were contoured. sMRI generated choline/N-acetylaspartate > 2x (Cho/NAA > 2x) volumes are known to correlate with high-risk invasion. Hausdorff distances were calculated to define the margin necessary to cover Cho/NAA > 2x in pGBM and rGBM. In rGBM, mock CTV expansions from T1PC volumes were created to determine non-selective CTV expansion sizes needed to cover Cho/NAA > 2x volumes.
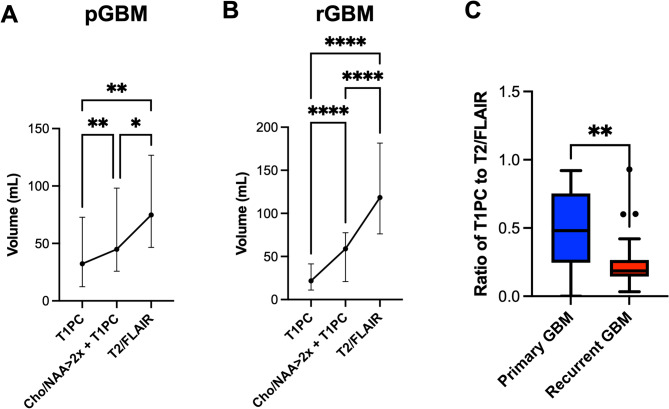
Results: For pGBM, the median T1PC, Cho/NAA > 2x, and T2/FLAIR volumes were 32.3 cc, 45.0 cc, and 74.8 cc respectively. For rGBM, the median T1PC, Cho/NAA > 2x, and T2/FLAIR volumes were 21.7 cc, 58.9 cc, and 118.3 cc, respectively. T2/FLAIR volumes increased more relative to T1PC volumes in rGBM than pGBM (p ≤ 0.001). Meanwhile, the median Hausdorff distance between T1PC and Cho/NAA > 2x was 22.9 mm in pGBM and 25.7 mm in rGBM, suggesting that the high-risk volume does not significantly change. In rGBM, it is common to use no CTV expansion from the T1PC volume which only included 61% of high-risk Cho/NAA > 2x volume. Conversely, T1PC expansions of 10-, 15-, and 20-mm covered 87%, 94%, and 98% of Cho/NAA > 2x volume.
Conclusions: sMRI Cho/NAA > 2x delineates high-risk occult disease in glioblastoma and extends beyond T1PC MRI borders. Typical large CTV expansions in pGBM mostly include Cho/NAA > 2x volumes. However, small CTV expansions commonly used in rGBM poorly cover Cho/NAA > 2x, suggesting that larger CTV expansions or Cho/NAA > 2x guidance may be of benefit.
Radiation OncologyONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
6.50
自引率
2.80%
发文量
181
审稿时长
3-6 weeks
期刊介绍:
Radiation Oncology encompasses all aspects of research that impacts on the treatment of cancer using radiation. It publishes findings in molecular and cellular radiation biology, radiation physics, radiation technology, and clinical oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


