Elena Kurz, Darius Kalasauskas, Dominik Wesp, Harald Krenzlin, Alicia Schulze, Melek Bulut, Thomas Kerz, Florian Ringel, Naureen Keric
{"title":"择期开颅术后必要的监测强度:对术后并发症进行分层监测的预测评分。","authors":"Elena Kurz, Darius Kalasauskas, Dominik Wesp, Harald Krenzlin, Alicia Schulze, Melek Bulut, Thomas Kerz, Florian Ringel, Naureen Keric","doi":"10.1007/s12028-025-02242-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postoperative complications requiring monitoring following elective craniotomies occur in ~ 2% of cases. Therefore, in most neurosurgical departments, an elective craniotomy is routinely followed by postoperative monitoring in an intensive or intermediate care unit. However, there is no systematic allocation to this procedure. Consequently, patients at risk are not monitored as a priority. The aim of this study was to develop a prediction score for the occurrence of postoperative complications after elective craniotomies and to redefine the monitoring algorithm.</p><p><strong>Methods: </strong>In this retrospective single-center analysis, all patients with elective craniotomy between 2018 and 2021 were included. Demographic data, diagnosis, location of the pathology (infratentorial/supratentorial), American Society of Anesthesiologists (ASA) score, Charlson comorbidity index (CCI), duration of surgery, blood loss, postoperative complications, and type and duration of monitoring were analyzed. The score was developed and validated internally to ensure its predictive reliability.</p><p><strong>Results: </strong>A total of 860 consecutive patients (376 male patients and 484 female patients) with a mean age of 60.6 years (range 19-93 years) were included. Forty-three patients experienced a postoperative adverse event that required monitoring. Independent predictors for postoperative complications were age (odds ratio [OR] 0.001, 95% confidence interval [CI] 1.0-1.04), CCI (OR 1.19, 95% CI 1.04-1.36), operative duration (OR 45.90, 95% CI 10.01-229.30), vestibular schwannoma as the treated pathology (OR 1.58, 95% CI 0.09-0.77), blood loss (OR 1.001, 95% CI 1.00-1.001), and ASA score (OR 1.1, 95% CI 1.01-1.2). The score was based on the most reliable characteristics and the calculated predictor error. The formula for score calculation is as follows: 1.3 age + 10 CCI + 65 1<sub>{vascular pathology = yes}</sub> + 0.5 duration of surgery + 20.5 ASA score - 100. The discriminatory value for clinical outcomes achieved an area under the curve of 0.78 in validation data.</p><p><strong>Conclusions: </strong>This score provides a practical approach for individual risk assessment of patients undergoing elective craniotomy. Postoperative monitoring capacity can be optimally distributed, and fast-track pathways can be developed for low-risk patients to use this valuable resource effectively.</p>","PeriodicalId":19118,"journal":{"name":"Neurocritical Care","volume":" ","pages":"484-492"},"PeriodicalIF":3.6000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436460/pdf/","citationCount":"0","resultStr":"{\"title\":\"Necessary Intensity of Monitoring After Elective Craniotomies: A Prediction Score for Postoperative Complications to Stratify Postoperative Monitoring.\",\"authors\":\"Elena Kurz, Darius Kalasauskas, Dominik Wesp, Harald Krenzlin, Alicia Schulze, Melek Bulut, Thomas Kerz, Florian Ringel, Naureen Keric\",\"doi\":\"10.1007/s12028-025-02242-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Postoperative complications requiring monitoring following elective craniotomies occur in ~ 2% of cases. Therefore, in most neurosurgical departments, an elective craniotomy is routinely followed by postoperative monitoring in an intensive or intermediate care unit. However, there is no systematic allocation to this procedure. Consequently, patients at risk are not monitored as a priority. The aim of this study was to develop a prediction score for the occurrence of postoperative complications after elective craniotomies and to redefine the monitoring algorithm.</p><p><strong>Methods: </strong>In this retrospective single-center analysis, all patients with elective craniotomy between 2018 and 2021 were included. Demographic data, diagnosis, location of the pathology (infratentorial/supratentorial), American Society of Anesthesiologists (ASA) score, Charlson comorbidity index (CCI), duration of surgery, blood loss, postoperative complications, and type and duration of monitoring were analyzed. The score was developed and validated internally to ensure its predictive reliability.</p><p><strong>Results: </strong>A total of 860 consecutive patients (376 male patients and 484 female patients) with a mean age of 60.6 years (range 19-93 years) were included. Forty-three patients experienced a postoperative adverse event that required monitoring. Independent predictors for postoperative complications were age (odds ratio [OR] 0.001, 95% confidence interval [CI] 1.0-1.04), CCI (OR 1.19, 95% CI 1.04-1.36), operative duration (OR 45.90, 95% CI 10.01-229.30), vestibular schwannoma as the treated pathology (OR 1.58, 95% CI 0.09-0.77), blood loss (OR 1.001, 95% CI 1.00-1.001), and ASA score (OR 1.1, 95% CI 1.01-1.2). The score was based on the most reliable characteristics and the calculated predictor error. The formula for score calculation is as follows: 1.3 age + 10 CCI + 65 1<sub>{vascular pathology = yes}</sub> + 0.5 duration of surgery + 20.5 ASA score - 100. The discriminatory value for clinical outcomes achieved an area under the curve of 0.78 in validation data.</p><p><strong>Conclusions: </strong>This score provides a practical approach for individual risk assessment of patients undergoing elective craniotomy. Postoperative monitoring capacity can be optimally distributed, and fast-track pathways can be developed for low-risk patients to use this valuable resource effectively.</p>\",\"PeriodicalId\":19118,\"journal\":{\"name\":\"Neurocritical Care\",\"volume\":\" \",\"pages\":\"484-492\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436460/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurocritical Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12028-025-02242-z\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurocritical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12028-025-02242-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:择期开颅手术后需要监测的术后并发症发生率约为2%。因此,在大多数神经外科,选择性开颅手术通常在重症监护病房或中级监护病房进行术后监测。但是,对这一程序没有系统的分配。因此,处于危险中的患者没有得到优先监测。本研究的目的是为择期开颅手术术后并发症的发生制定预测评分,并重新定义监测算法。方法:回顾性单中心分析纳入2018 - 2021年间所有择期开颅手术患者。分析人口学资料、诊断、病理部位(幕下/幕上)、美国麻醉医师学会(ASA)评分、Charlson合并症指数(CCI)、手术时间、出血量、术后并发症、监测类型和持续时间。该评分是内部开发和验证的,以确保其预测可靠性。结果:共纳入连续860例患者,其中男性376例,女性484例,平均年龄60.6岁(范围19-93岁)。43例患者出现了需要监测的术后不良事件。术后并发症的独立预测因素为年龄(比值比[OR] 0.001, 95%可信区间[CI] 1.0-1.04)、CCI (OR 1.19, 95% CI 1.04-1.36)、手术时间(OR 45.90, 95% CI 10.01-229.30)、前庭神经鞘瘤作为治疗病理(OR 1.58, 95% CI 0.09-0.77)、出血量(OR 1.001, 95% CI 1.00-1.001)和ASA评分(OR 1.1, 95% CI 1.01-1.2)。评分是基于最可靠的特征和计算的预测误差。评分计算公式为:1.3年龄+ 10 CCI + 65 1{血管病理= yes} + 0.5手术时间+ 20.5 ASA评分- 100。在验证数据中,临床结果的鉴别值达到曲线下面积0.78。结论:该评分为择期开颅手术患者的个体风险评估提供了实用的方法。术后监测能力可以优化分配,为低风险患者开发快速通道,有效利用这一宝贵资源。
Necessary Intensity of Monitoring After Elective Craniotomies: A Prediction Score for Postoperative Complications to Stratify Postoperative Monitoring.
Background: Postoperative complications requiring monitoring following elective craniotomies occur in ~ 2% of cases. Therefore, in most neurosurgical departments, an elective craniotomy is routinely followed by postoperative monitoring in an intensive or intermediate care unit. However, there is no systematic allocation to this procedure. Consequently, patients at risk are not monitored as a priority. The aim of this study was to develop a prediction score for the occurrence of postoperative complications after elective craniotomies and to redefine the monitoring algorithm.
Methods: In this retrospective single-center analysis, all patients with elective craniotomy between 2018 and 2021 were included. Demographic data, diagnosis, location of the pathology (infratentorial/supratentorial), American Society of Anesthesiologists (ASA) score, Charlson comorbidity index (CCI), duration of surgery, blood loss, postoperative complications, and type and duration of monitoring were analyzed. The score was developed and validated internally to ensure its predictive reliability.
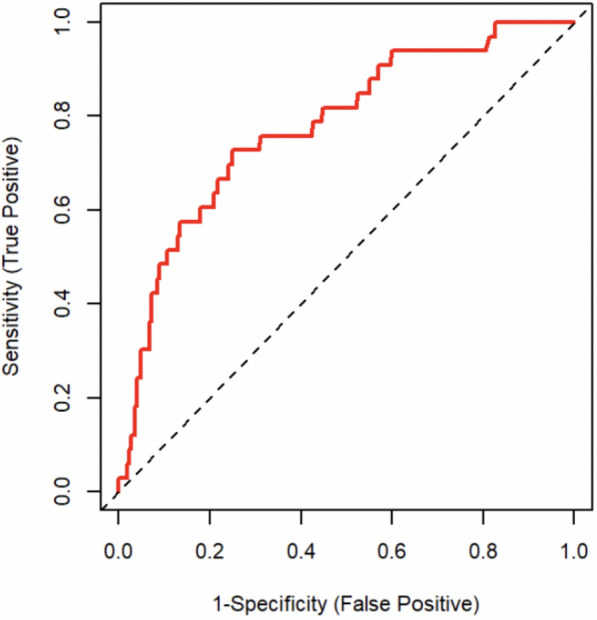
Results: A total of 860 consecutive patients (376 male patients and 484 female patients) with a mean age of 60.6 years (range 19-93 years) were included. Forty-three patients experienced a postoperative adverse event that required monitoring. Independent predictors for postoperative complications were age (odds ratio [OR] 0.001, 95% confidence interval [CI] 1.0-1.04), CCI (OR 1.19, 95% CI 1.04-1.36), operative duration (OR 45.90, 95% CI 10.01-229.30), vestibular schwannoma as the treated pathology (OR 1.58, 95% CI 0.09-0.77), blood loss (OR 1.001, 95% CI 1.00-1.001), and ASA score (OR 1.1, 95% CI 1.01-1.2). The score was based on the most reliable characteristics and the calculated predictor error. The formula for score calculation is as follows: 1.3 age + 10 CCI + 65 1{vascular pathology = yes} + 0.5 duration of surgery + 20.5 ASA score - 100. The discriminatory value for clinical outcomes achieved an area under the curve of 0.78 in validation data.
Conclusions: This score provides a practical approach for individual risk assessment of patients undergoing elective craniotomy. Postoperative monitoring capacity can be optimally distributed, and fast-track pathways can be developed for low-risk patients to use this valuable resource effectively.
期刊介绍:
Neurocritical Care is a peer reviewed scientific publication whose major goal is to disseminate new knowledge on all aspects of acute neurological care. It is directed towards neurosurgeons, neuro-intensivists, neurologists, anesthesiologists, emergency physicians, and critical care nurses treating patients with urgent neurologic disorders. These are conditions that may potentially evolve rapidly and could need immediate medical or surgical intervention. Neurocritical Care provides a comprehensive overview of current developments in intensive care neurology, neurosurgery and neuroanesthesia and includes information about new therapeutic avenues and technological innovations. Neurocritical Care is the official journal of the Neurocritical Care Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


