Min-Yi Cheng, Can-Gui Wu, Ying-Yi Lin, Jia-Chen Zou, Dong-Qing Wang, Bruce G Haffty, Kun Wang
{"title":"基于临床病理特征、乳房x光检查和MRI成像特征的多变量风险模型的建立和验证,用于预测升级型导管原位癌患者腋窝淋巴结转移。","authors":"Min-Yi Cheng, Can-Gui Wu, Ying-Yi Lin, Jia-Chen Zou, Dong-Qing Wang, Bruce G Haffty, Kun Wang","doi":"10.21037/gs-2025-89","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Axillary surgical staging is required for patients with upgraded ductal carcinoma in situ (DCIS) (DCIS is diagnosed on core biopsy with invasive cancer found on pathology after complete surgical excision), which may lead to complications in axillary surgery. At present, there is no reliable and accurate method for predicting axillary lymph node metastasis (ALNM) in patients with upgraded DCIS; however, such a method could prevent unnecessary axillary surgical interventions from being performed. In this study, we aimed to construct a non-invasive model for predicting ALNM in DCIS patients based on clinicopathological characteristics, mammography (MG) features, and magnetic resonance imaging (MRI) features.</p><p><strong>Methods: </strong>Between February 2018 and June 2020, 326 patients with upgraded DCIS were enrolled in this retrospective analysis. These patients were randomly divided into the training cohort (80%) and validation cohort (20%). Univariate and multivariable regression analyses were conducted to identify the candidate pathological features, which then used to develop a clinicopathological model. The features of the 2-mm, 4-mm, and 6-mm intratumoral and peritumoral regions (T-PTR) were extracted to develop the MRI radiomics model, and two deep learning classification models were developed based on the medial-lateral oblique (MLO) and craniocaudal (CC) views of the MG. A fusion model was then established that combined these sub-models. The receiver operating characteristic (ROC) curve, area under the curve (AUC), and other indicators were used to evaluate the performance of these models.</p><p><strong>Results: </strong>The clinicopathological characteristics of the two cohorts were basically balanced. The AUC values of the clinicopathological model were 0.675 and 0.690 in the training and validation cohorts, respectively. The model based on the T-PTR of MRI showed promising predictive ability. Among the three MRI models, the T-PTR (4 mm) model showed the best predictivity both in the training (AUC =0.885) and validation cohorts (AUC =0.843). The AUC values for the deep learning models of the MG CC and MLO positions all exceeded 0.7, indicating reliable predictive performance. The fusion model that combined the three methods significantly improved the accuracy and robustness of ALNM prediction. In both the training (AUC =0.975) and validation (AUC =0.877) cohorts, the fusion model showed excellent performance.</p><p><strong>Conclusions: </strong>We developed a fusion model that combined clinicopathological characteristics, MRI T-PTR (4 mm) radiomics, and MG-based deep learning. Our combined model showed promising performance in predicting ALNM in patients with upgraded DCIS.</p>","PeriodicalId":12760,"journal":{"name":"Gland surgery","volume":"14 4","pages":"738-753"},"PeriodicalIF":1.6000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12093168/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development and validation of a multivariable risk model based on clinicopathological characteristics, mammography, and MRI imaging features for predicting axillary lymph node metastasis in patients with upgraded ductal carcinoma <i>in situ</i>.\",\"authors\":\"Min-Yi Cheng, Can-Gui Wu, Ying-Yi Lin, Jia-Chen Zou, Dong-Qing Wang, Bruce G Haffty, Kun Wang\",\"doi\":\"10.21037/gs-2025-89\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Axillary surgical staging is required for patients with upgraded ductal carcinoma in situ (DCIS) (DCIS is diagnosed on core biopsy with invasive cancer found on pathology after complete surgical excision), which may lead to complications in axillary surgery. At present, there is no reliable and accurate method for predicting axillary lymph node metastasis (ALNM) in patients with upgraded DCIS; however, such a method could prevent unnecessary axillary surgical interventions from being performed. In this study, we aimed to construct a non-invasive model for predicting ALNM in DCIS patients based on clinicopathological characteristics, mammography (MG) features, and magnetic resonance imaging (MRI) features.</p><p><strong>Methods: </strong>Between February 2018 and June 2020, 326 patients with upgraded DCIS were enrolled in this retrospective analysis. These patients were randomly divided into the training cohort (80%) and validation cohort (20%). Univariate and multivariable regression analyses were conducted to identify the candidate pathological features, which then used to develop a clinicopathological model. The features of the 2-mm, 4-mm, and 6-mm intratumoral and peritumoral regions (T-PTR) were extracted to develop the MRI radiomics model, and two deep learning classification models were developed based on the medial-lateral oblique (MLO) and craniocaudal (CC) views of the MG. A fusion model was then established that combined these sub-models. The receiver operating characteristic (ROC) curve, area under the curve (AUC), and other indicators were used to evaluate the performance of these models.</p><p><strong>Results: </strong>The clinicopathological characteristics of the two cohorts were basically balanced. The AUC values of the clinicopathological model were 0.675 and 0.690 in the training and validation cohorts, respectively. The model based on the T-PTR of MRI showed promising predictive ability. Among the three MRI models, the T-PTR (4 mm) model showed the best predictivity both in the training (AUC =0.885) and validation cohorts (AUC =0.843). The AUC values for the deep learning models of the MG CC and MLO positions all exceeded 0.7, indicating reliable predictive performance. The fusion model that combined the three methods significantly improved the accuracy and robustness of ALNM prediction. In both the training (AUC =0.975) and validation (AUC =0.877) cohorts, the fusion model showed excellent performance.</p><p><strong>Conclusions: </strong>We developed a fusion model that combined clinicopathological characteristics, MRI T-PTR (4 mm) radiomics, and MG-based deep learning. Our combined model showed promising performance in predicting ALNM in patients with upgraded DCIS.</p>\",\"PeriodicalId\":12760,\"journal\":{\"name\":\"Gland surgery\",\"volume\":\"14 4\",\"pages\":\"738-753\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12093168/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gland surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/gs-2025-89\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gland surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/gs-2025-89","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Development and validation of a multivariable risk model based on clinicopathological characteristics, mammography, and MRI imaging features for predicting axillary lymph node metastasis in patients with upgraded ductal carcinoma in situ.
Background: Axillary surgical staging is required for patients with upgraded ductal carcinoma in situ (DCIS) (DCIS is diagnosed on core biopsy with invasive cancer found on pathology after complete surgical excision), which may lead to complications in axillary surgery. At present, there is no reliable and accurate method for predicting axillary lymph node metastasis (ALNM) in patients with upgraded DCIS; however, such a method could prevent unnecessary axillary surgical interventions from being performed. In this study, we aimed to construct a non-invasive model for predicting ALNM in DCIS patients based on clinicopathological characteristics, mammography (MG) features, and magnetic resonance imaging (MRI) features.
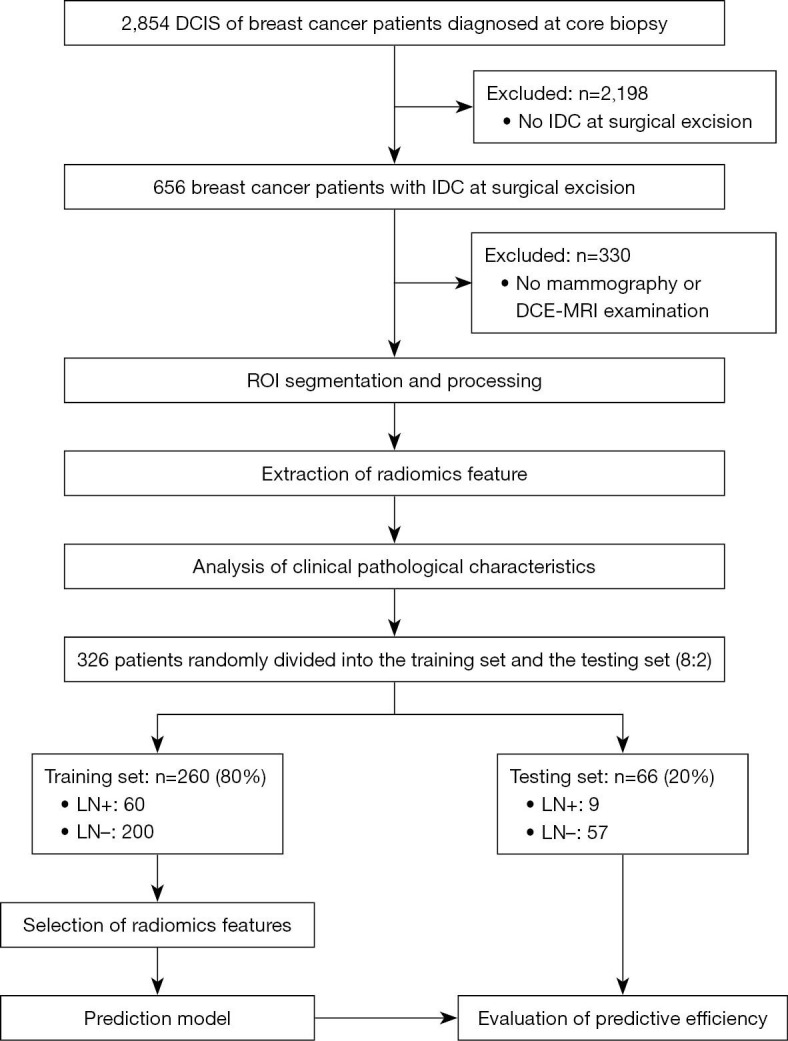
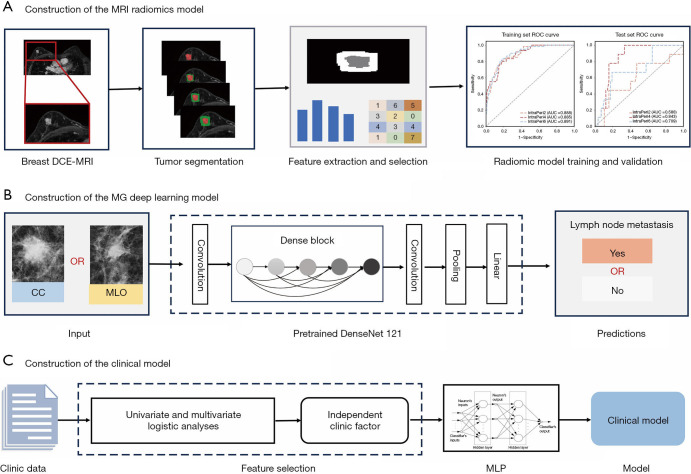
Methods: Between February 2018 and June 2020, 326 patients with upgraded DCIS were enrolled in this retrospective analysis. These patients were randomly divided into the training cohort (80%) and validation cohort (20%). Univariate and multivariable regression analyses were conducted to identify the candidate pathological features, which then used to develop a clinicopathological model. The features of the 2-mm, 4-mm, and 6-mm intratumoral and peritumoral regions (T-PTR) were extracted to develop the MRI radiomics model, and two deep learning classification models were developed based on the medial-lateral oblique (MLO) and craniocaudal (CC) views of the MG. A fusion model was then established that combined these sub-models. The receiver operating characteristic (ROC) curve, area under the curve (AUC), and other indicators were used to evaluate the performance of these models.
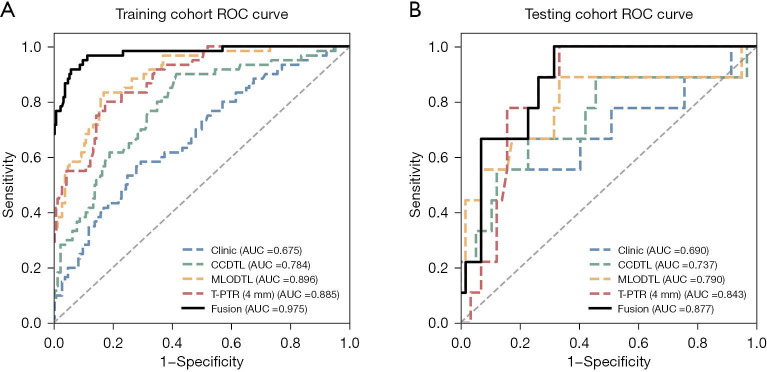
Results: The clinicopathological characteristics of the two cohorts were basically balanced. The AUC values of the clinicopathological model were 0.675 and 0.690 in the training and validation cohorts, respectively. The model based on the T-PTR of MRI showed promising predictive ability. Among the three MRI models, the T-PTR (4 mm) model showed the best predictivity both in the training (AUC =0.885) and validation cohorts (AUC =0.843). The AUC values for the deep learning models of the MG CC and MLO positions all exceeded 0.7, indicating reliable predictive performance. The fusion model that combined the three methods significantly improved the accuracy and robustness of ALNM prediction. In both the training (AUC =0.975) and validation (AUC =0.877) cohorts, the fusion model showed excellent performance.
Conclusions: We developed a fusion model that combined clinicopathological characteristics, MRI T-PTR (4 mm) radiomics, and MG-based deep learning. Our combined model showed promising performance in predicting ALNM in patients with upgraded DCIS.
期刊介绍:
Gland Surgery (Gland Surg; GS, Print ISSN 2227-684X; Online ISSN 2227-8575) being indexed by PubMed/PubMed Central, is an open access, peer-review journal launched at May of 2012, published bio-monthly since February 2015.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


