{"title":"慢性肛裂的治疗:是否应该注射肉毒杆菌毒素进行肛裂切除术?","authors":"R Quinn, J Ellis-Clark, S Albayati","doi":"10.1007/s10151-025-03153-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite the superior success rate of lateral internal sphincterotomy for managing chronic anal fissure (CAF), there is a trend towards sphincter-preserving treatment due to the increased risk of incontinence. Botulinum toxin (BT) and fissurectomy are two sphincter-preserving options for CAF. We aim to assess if combining fissurectomy with botox treatment is superior to botulinum toxin alone in the management of CAF.</p><p><strong>Methods: </strong>This retrospective cohort study was conducted across two Sydney hospitals over 7 years. All patients with a CAF managed with either BT and fissurectomy (group 1) or BT only (group 2) were included. Primary outcome was healing rate defined as resolution or significant improvement of perianal symptoms at initial follow-up. Secondary outcomes were persistence, recurrence, re-intervention and faecal incontinence rate. Follow-up questionnaire was conducted to compare long-term outcomes between the two groups.</p><p><strong>Results: </strong>Fifty-seven patients met the inclusion criteria (group 1, 37; group 2, 20). Mean BT dose and injection location between the groups were similar (p = 0.259 and p = 0.427). There was a 65% response rate to the follow-up questionnaire. Median follow-up was 34.3 months (range 0.4-93). There was no difference in healing (56.7% vs. 50%, p = 0.561), recurrence (37.8% vs. 30%, p = 0.383) or re-intervention rate (13.5% vs. 20%, p = 0.888). Long-term incontinence rate was significantly higher in patients group 2 (0% vs. 10%, p = 0.010), with two patients reporting persistent flatus incontinence. Median overall satisfaction score was 3/4 (range 1-4), in both groups (p = 0.469).</p><p><strong>Conclusion: </strong>Botulinum toxin with or without fissurectomy is a safe sphincter-sparing treatment option for CAF. However, the addition of fissurectomy to BT does not improve healing rates and we therefore recommend BT injection alone as a second-line treatment of CAF in patients who fail topical treatment.</p>","PeriodicalId":51192,"journal":{"name":"Techniques in Coloproctology","volume":"29 1","pages":"118"},"PeriodicalIF":2.9000,"publicationDate":"2025-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12098196/pdf/","citationCount":"0","resultStr":"{\"title\":\"Management of chronic anal fissures: should fissurectomy be performed with botulinum toxin injection?\",\"authors\":\"R Quinn, J Ellis-Clark, S Albayati\",\"doi\":\"10.1007/s10151-025-03153-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Despite the superior success rate of lateral internal sphincterotomy for managing chronic anal fissure (CAF), there is a trend towards sphincter-preserving treatment due to the increased risk of incontinence. Botulinum toxin (BT) and fissurectomy are two sphincter-preserving options for CAF. We aim to assess if combining fissurectomy with botox treatment is superior to botulinum toxin alone in the management of CAF.</p><p><strong>Methods: </strong>This retrospective cohort study was conducted across two Sydney hospitals over 7 years. All patients with a CAF managed with either BT and fissurectomy (group 1) or BT only (group 2) were included. Primary outcome was healing rate defined as resolution or significant improvement of perianal symptoms at initial follow-up. Secondary outcomes were persistence, recurrence, re-intervention and faecal incontinence rate. Follow-up questionnaire was conducted to compare long-term outcomes between the two groups.</p><p><strong>Results: </strong>Fifty-seven patients met the inclusion criteria (group 1, 37; group 2, 20). Mean BT dose and injection location between the groups were similar (p = 0.259 and p = 0.427). There was a 65% response rate to the follow-up questionnaire. Median follow-up was 34.3 months (range 0.4-93). There was no difference in healing (56.7% vs. 50%, p = 0.561), recurrence (37.8% vs. 30%, p = 0.383) or re-intervention rate (13.5% vs. 20%, p = 0.888). Long-term incontinence rate was significantly higher in patients group 2 (0% vs. 10%, p = 0.010), with two patients reporting persistent flatus incontinence. Median overall satisfaction score was 3/4 (range 1-4), in both groups (p = 0.469).</p><p><strong>Conclusion: </strong>Botulinum toxin with or without fissurectomy is a safe sphincter-sparing treatment option for CAF. However, the addition of fissurectomy to BT does not improve healing rates and we therefore recommend BT injection alone as a second-line treatment of CAF in patients who fail topical treatment.</p>\",\"PeriodicalId\":51192,\"journal\":{\"name\":\"Techniques in Coloproctology\",\"volume\":\"29 1\",\"pages\":\"118\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-05-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12098196/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Techniques in Coloproctology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10151-025-03153-z\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Techniques in Coloproctology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10151-025-03153-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:尽管外侧内括约肌切开术治疗慢性肛裂(CAF)的成功率较高,但由于尿失禁的风险增加,保留括约肌的治疗有趋势。肉毒杆菌毒素(BT)和裂切除是两种保留括约肌的选择。我们的目的是评估在CAF的治疗中,裂裂切除联合肉毒杆菌毒素治疗是否优于单独使用肉毒杆菌毒素治疗。方法:这项回顾性队列研究在悉尼两家医院进行了7年。所有CAF患者均采用BT和裂切术(组1)或仅采用BT(组2)。主要终点是治愈率,定义为初次随访时肛周症状的缓解或显著改善。次要结局是持续、复发、再干预和大便失禁率。通过随访问卷比较两组患者的远期疗效。结果:57例患者符合纳入标准(1、37组;第2,20组)。各组间BT平均剂量和注射部位相似(p = 0.259和p = 0.427)。随访问卷的回复率为65%。中位随访时间为34.3个月(范围0.4-93)。两组患者的治愈率(56.7%比50%,p = 0.561)、复发率(37.8%比30%,p = 0.383)、再干预率(13.5%比20%,p = 0.888)差异无统计学意义。患者2组的长期失禁率显著高于对照组(0% vs. 10%, p = 0.010),其中2例患者报告持续性肠胃失禁。两组总体满意度中位数均为3/4(范围1-4)(p = 0.469)。结论:肉毒杆菌毒素联合或不联合裂切除是一种安全的保括约肌治疗CAF的选择。然而,除了BT外,裂隙切除术并不能提高治愈率,因此我们建议局部治疗失败的患者单独注射BT作为CAF的二线治疗。
Management of chronic anal fissures: should fissurectomy be performed with botulinum toxin injection?
Background: Despite the superior success rate of lateral internal sphincterotomy for managing chronic anal fissure (CAF), there is a trend towards sphincter-preserving treatment due to the increased risk of incontinence. Botulinum toxin (BT) and fissurectomy are two sphincter-preserving options for CAF. We aim to assess if combining fissurectomy with botox treatment is superior to botulinum toxin alone in the management of CAF.
Methods: This retrospective cohort study was conducted across two Sydney hospitals over 7 years. All patients with a CAF managed with either BT and fissurectomy (group 1) or BT only (group 2) were included. Primary outcome was healing rate defined as resolution or significant improvement of perianal symptoms at initial follow-up. Secondary outcomes were persistence, recurrence, re-intervention and faecal incontinence rate. Follow-up questionnaire was conducted to compare long-term outcomes between the two groups.
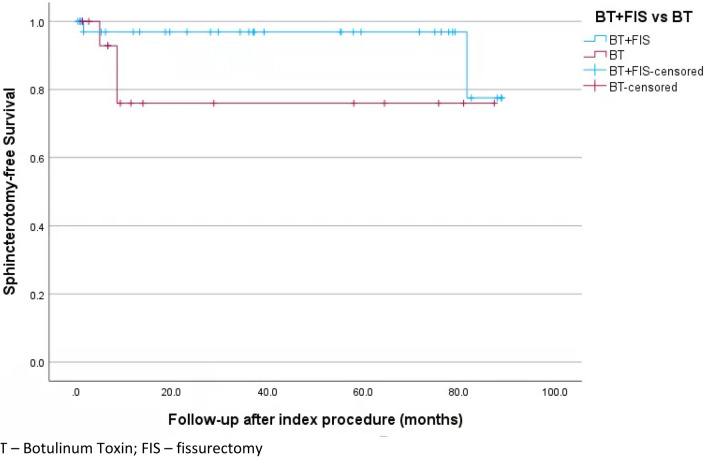
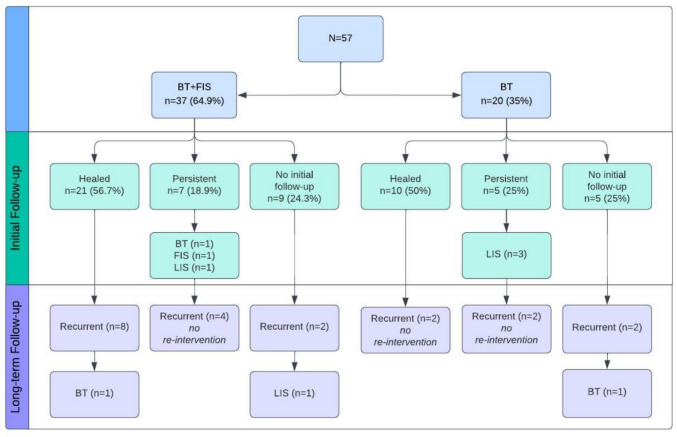
Results: Fifty-seven patients met the inclusion criteria (group 1, 37; group 2, 20). Mean BT dose and injection location between the groups were similar (p = 0.259 and p = 0.427). There was a 65% response rate to the follow-up questionnaire. Median follow-up was 34.3 months (range 0.4-93). There was no difference in healing (56.7% vs. 50%, p = 0.561), recurrence (37.8% vs. 30%, p = 0.383) or re-intervention rate (13.5% vs. 20%, p = 0.888). Long-term incontinence rate was significantly higher in patients group 2 (0% vs. 10%, p = 0.010), with two patients reporting persistent flatus incontinence. Median overall satisfaction score was 3/4 (range 1-4), in both groups (p = 0.469).
Conclusion: Botulinum toxin with or without fissurectomy is a safe sphincter-sparing treatment option for CAF. However, the addition of fissurectomy to BT does not improve healing rates and we therefore recommend BT injection alone as a second-line treatment of CAF in patients who fail topical treatment.
期刊介绍:
Techniques in Coloproctology is an international journal fully devoted to diagnostic and operative procedures carried out in the management of colorectal diseases. Imaging, clinical physiology, laparoscopy, open abdominal surgery and proctoperineology are the main topics covered by the journal. Reviews, original articles, technical notes and short communications with many detailed illustrations render this publication indispensable for coloproctologists and related specialists. Both surgeons and gastroenterologists are represented on the distinguished Editorial Board, together with pathologists, radiologists and basic scientists from all over the world. The journal is strongly recommended to those who wish to be updated on recent developments in the field, and improve the standards of their work.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1965 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted. Reports of animal experiments must state that the Principles of Laboratory Animal Care (NIH publication no. 86-23 revised 1985) were followed as were applicable national laws (e.g. the current version of the German Law on the Protection of Animals). The Editor-in-Chief reserves the right to reject manuscripts that do not comply with the above-mentioned requirements. Authors will be held responsible for false statements or for failure to fulfill such requirements.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


