Elizabeth Squirell, Gregory Rosenfeld, Brian Bressler, Susanna Meade, Natasha Klemm, Victoria Chen, Elisabet Joa, Yvette Leung
{"title":"怀孕暂停?不适合IBD治疗——单一三级保健中心前瞻性队列研究证实妊娠期IBD治疗。","authors":"Elizabeth Squirell, Gregory Rosenfeld, Brian Bressler, Susanna Meade, Natasha Klemm, Victoria Chen, Elisabet Joa, Yvette Leung","doi":"10.1093/crocol/otaf029","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study examined Inflammatory Bowel Disease (IBD) management and outcomes during pregnancy in a tertiary care setting, focusing on disease activity, medication use, and maternal and neonatal outcomes.</p><p><strong>Methods: </strong>A prospective cohort study followed 287 women with IBD through 291 pregnancies from 2017 to 2023 at a single tertiary care center, collecting data preconception, during each trimester, and postpartum.</p><p><strong>Results: </strong>The study observed a 92.7% live birth rate. Seventy-four percent of individuals were in clinical remission preconception, and disease activity increased throughout pregnancy, particularly in ulcerative colitis (UC) patients (peaking at 37% in the second trimester), while remaining stable in CD patients. UC, disease duration <5 years, and preconception activity correlated with higher disease activity during pregnancy. Biologic use remained stable without significant impact on outcomes. Preterm delivery (6.7%) and small for gestational age infants (7%) rates reflected baseline population risk. Steroid use was associated with higher preterm delivery rates. Gestational hypertension (6.9%) and diabetes (9.4%) rates were similar to population norms. Maternal adverse events were higher in women 40 or older (OR 3.893).</p><p><strong>Conclusions: </strong>This study reaffirms the safety of continued medical therapy for IBD throughout pregnancy in a tertiary care, prospective cohort. Increased disease activity throughout pregnancy was evident, particularly in UC. Despite higher rates of disease activity amongst those with UC, outcomes were similar in those with CD vs UC-suggesting that disease activity measures have limitations in CD and pregnancy, or there is some mild inherent risk of CD in pregnancy outcomes irrespective of disease activity.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"7 2","pages":"otaf029"},"PeriodicalIF":1.8000,"publicationDate":"2025-04-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12093221/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pregnant Pause? Not for IBD Care-A Single Tertiary Care Center Prospective Cohort Study Affirming IBD Management in Pregnancy.\",\"authors\":\"Elizabeth Squirell, Gregory Rosenfeld, Brian Bressler, Susanna Meade, Natasha Klemm, Victoria Chen, Elisabet Joa, Yvette Leung\",\"doi\":\"10.1093/crocol/otaf029\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study examined Inflammatory Bowel Disease (IBD) management and outcomes during pregnancy in a tertiary care setting, focusing on disease activity, medication use, and maternal and neonatal outcomes.</p><p><strong>Methods: </strong>A prospective cohort study followed 287 women with IBD through 291 pregnancies from 2017 to 2023 at a single tertiary care center, collecting data preconception, during each trimester, and postpartum.</p><p><strong>Results: </strong>The study observed a 92.7% live birth rate. Seventy-four percent of individuals were in clinical remission preconception, and disease activity increased throughout pregnancy, particularly in ulcerative colitis (UC) patients (peaking at 37% in the second trimester), while remaining stable in CD patients. UC, disease duration <5 years, and preconception activity correlated with higher disease activity during pregnancy. Biologic use remained stable without significant impact on outcomes. Preterm delivery (6.7%) and small for gestational age infants (7%) rates reflected baseline population risk. Steroid use was associated with higher preterm delivery rates. Gestational hypertension (6.9%) and diabetes (9.4%) rates were similar to population norms. Maternal adverse events were higher in women 40 or older (OR 3.893).</p><p><strong>Conclusions: </strong>This study reaffirms the safety of continued medical therapy for IBD throughout pregnancy in a tertiary care, prospective cohort. Increased disease activity throughout pregnancy was evident, particularly in UC. Despite higher rates of disease activity amongst those with UC, outcomes were similar in those with CD vs UC-suggesting that disease activity measures have limitations in CD and pregnancy, or there is some mild inherent risk of CD in pregnancy outcomes irrespective of disease activity.</p>\",\"PeriodicalId\":10847,\"journal\":{\"name\":\"Crohn's & Colitis 360\",\"volume\":\"7 2\",\"pages\":\"otaf029\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-04-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12093221/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Crohn's & Colitis 360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/crocol/otaf029\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otaf029","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Pregnant Pause? Not for IBD Care-A Single Tertiary Care Center Prospective Cohort Study Affirming IBD Management in Pregnancy.
Background: This study examined Inflammatory Bowel Disease (IBD) management and outcomes during pregnancy in a tertiary care setting, focusing on disease activity, medication use, and maternal and neonatal outcomes.
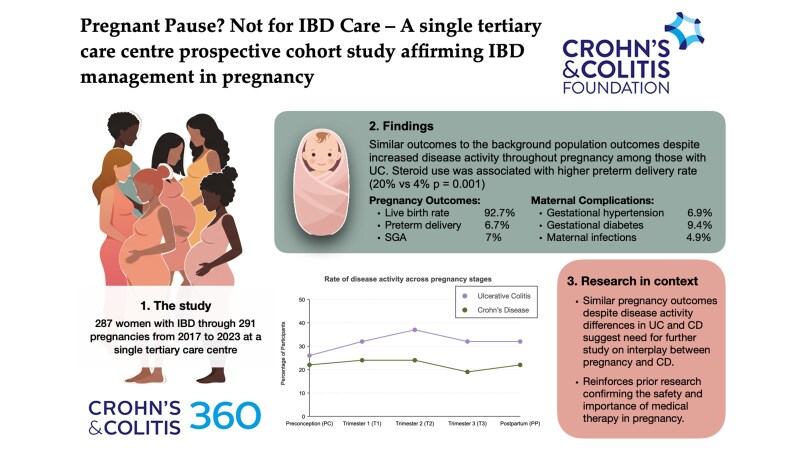
Methods: A prospective cohort study followed 287 women with IBD through 291 pregnancies from 2017 to 2023 at a single tertiary care center, collecting data preconception, during each trimester, and postpartum.
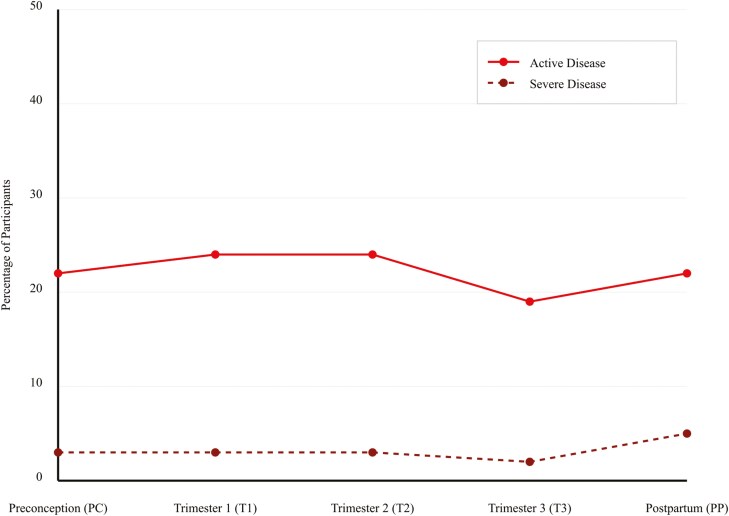
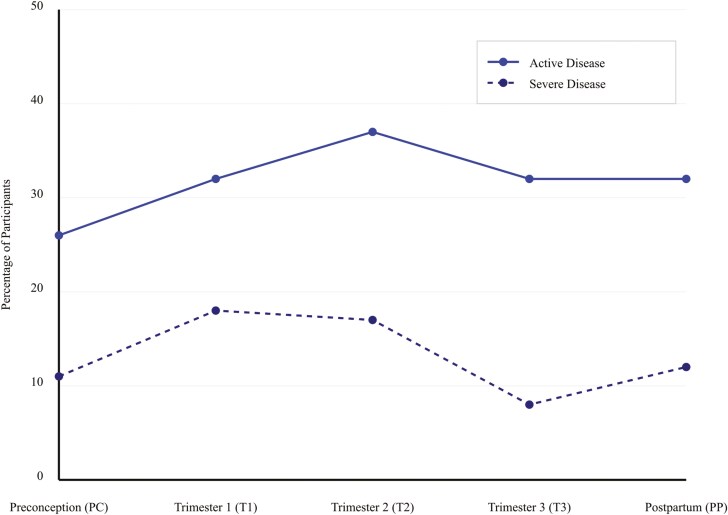
Results: The study observed a 92.7% live birth rate. Seventy-four percent of individuals were in clinical remission preconception, and disease activity increased throughout pregnancy, particularly in ulcerative colitis (UC) patients (peaking at 37% in the second trimester), while remaining stable in CD patients. UC, disease duration <5 years, and preconception activity correlated with higher disease activity during pregnancy. Biologic use remained stable without significant impact on outcomes. Preterm delivery (6.7%) and small for gestational age infants (7%) rates reflected baseline population risk. Steroid use was associated with higher preterm delivery rates. Gestational hypertension (6.9%) and diabetes (9.4%) rates were similar to population norms. Maternal adverse events were higher in women 40 or older (OR 3.893).
Conclusions: This study reaffirms the safety of continued medical therapy for IBD throughout pregnancy in a tertiary care, prospective cohort. Increased disease activity throughout pregnancy was evident, particularly in UC. Despite higher rates of disease activity amongst those with UC, outcomes were similar in those with CD vs UC-suggesting that disease activity measures have limitations in CD and pregnancy, or there is some mild inherent risk of CD in pregnancy outcomes irrespective of disease activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


