{"title":"来自日本的真实证据,关于接受CDK4/6抑制剂加内分泌治疗作为激素受体阳性、her2阴性晚期或转移性乳腺癌一线或二线治疗的患者的生存结局和治疗顺序。","authors":"Tetsuhiro Yoshinami, Yuko Takano, Yukinori Ozaki, Yukiko Kajiwara, Mitsugu Yamamoto, Ken-Ichi Watanabe, Masami Tsukabe, Fumie Fujisawa, Shigenori E Nagai, Nobuhiro Shibata, Chiya Oshiro, Hiroko Bando, Nobuyuki Tsunoda, Kazuhiko Yamagami, Kei Koizumi, Masahiro Takada, Naoko Toriguchi, Nobuyuki Sekine, Tsutomu Kawaguchi, Shigehira Saji, Yasuaki Sagara, Satoshi Morita, Norikazu Masuda","doi":"10.1007/s12282-025-01713-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) plus endocrine therapy (ET) is a current standard first-/second-line treatment for hormone receptor (HR)-positive, HER2-negative advanced/metastatic breast cancer (AMBC). We aimed to provide real-world evidence regarding CDK4/6i therapy in this population.</p><p><strong>Methods: </strong>In this multicenter observational study, data from patients who had started CDK4/6i therapy between January 1, 2019, and December 31, 2021, as first-/second-line treatment for AMBC were used; real-world progression-free survival (rwPFS), chemotherapy-free survival, and overall survival were analyzed using the Kaplan-Meier method. Additionally, data were analyzed by separating patients with treatment-free interval (TFI) < 12 months (deemed resistant to ET) from the first-line treatment group (hereafter, the exclusive first-line treatment group).</p><p><strong>Results: </strong>Data from 745 patients were analyzed. Compared with palbociclib, abemaciclib was used in younger patients and those with expected poor prognosis. Median rwPFS was 36.8, 17.8, and 31.4 months in patients with de novo stage IV disease, TFI < 12 months, and TFI ≥ 12 months, respectively, in the first-line treatment group, and 17.4 months in the second-line treatment group. In the exclusive first-line treatment group, median rwPFS of the subsequent treatment after initial CDK4/6i plus ET was < 7 months, regardless of the type of subsequent treatment; prognosis was especially poor in those who were switched to chemotherapy.</p><p><strong>Conclusions: </strong>The real-world survival outcomes found in this study for patients receiving first-/second-line CDK4/6i therapy were consistent with those of randomized phase 3 studies. As outcomes of subsequent treatment after initial CDK4/6i plus ET remain insufficient, further improvement in treatment is necessary.</p>","PeriodicalId":520574,"journal":{"name":"Breast cancer (Tokyo, Japan)","volume":" ","pages":"841-856"},"PeriodicalIF":2.9000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12174191/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-world evidence from Japan regarding survival outcomes and treatment sequence in patients receiving CDK4/6 inhibitor plus endocrine therapy as first- or second-line treatment for hormone receptor-positive, HER2-negative advanced or metastatic breast cancer.\",\"authors\":\"Tetsuhiro Yoshinami, Yuko Takano, Yukinori Ozaki, Yukiko Kajiwara, Mitsugu Yamamoto, Ken-Ichi Watanabe, Masami Tsukabe, Fumie Fujisawa, Shigenori E Nagai, Nobuhiro Shibata, Chiya Oshiro, Hiroko Bando, Nobuyuki Tsunoda, Kazuhiko Yamagami, Kei Koizumi, Masahiro Takada, Naoko Toriguchi, Nobuyuki Sekine, Tsutomu Kawaguchi, Shigehira Saji, Yasuaki Sagara, Satoshi Morita, Norikazu Masuda\",\"doi\":\"10.1007/s12282-025-01713-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) plus endocrine therapy (ET) is a current standard first-/second-line treatment for hormone receptor (HR)-positive, HER2-negative advanced/metastatic breast cancer (AMBC). We aimed to provide real-world evidence regarding CDK4/6i therapy in this population.</p><p><strong>Methods: </strong>In this multicenter observational study, data from patients who had started CDK4/6i therapy between January 1, 2019, and December 31, 2021, as first-/second-line treatment for AMBC were used; real-world progression-free survival (rwPFS), chemotherapy-free survival, and overall survival were analyzed using the Kaplan-Meier method. Additionally, data were analyzed by separating patients with treatment-free interval (TFI) < 12 months (deemed resistant to ET) from the first-line treatment group (hereafter, the exclusive first-line treatment group).</p><p><strong>Results: </strong>Data from 745 patients were analyzed. Compared with palbociclib, abemaciclib was used in younger patients and those with expected poor prognosis. Median rwPFS was 36.8, 17.8, and 31.4 months in patients with de novo stage IV disease, TFI < 12 months, and TFI ≥ 12 months, respectively, in the first-line treatment group, and 17.4 months in the second-line treatment group. In the exclusive first-line treatment group, median rwPFS of the subsequent treatment after initial CDK4/6i plus ET was < 7 months, regardless of the type of subsequent treatment; prognosis was especially poor in those who were switched to chemotherapy.</p><p><strong>Conclusions: </strong>The real-world survival outcomes found in this study for patients receiving first-/second-line CDK4/6i therapy were consistent with those of randomized phase 3 studies. As outcomes of subsequent treatment after initial CDK4/6i plus ET remain insufficient, further improvement in treatment is necessary.</p>\",\"PeriodicalId\":520574,\"journal\":{\"name\":\"Breast cancer (Tokyo, Japan)\",\"volume\":\" \",\"pages\":\"841-856\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12174191/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Breast cancer (Tokyo, Japan)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s12282-025-01713-7\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast cancer (Tokyo, Japan)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12282-025-01713-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/20 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Real-world evidence from Japan regarding survival outcomes and treatment sequence in patients receiving CDK4/6 inhibitor plus endocrine therapy as first- or second-line treatment for hormone receptor-positive, HER2-negative advanced or metastatic breast cancer.
Background: A cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) plus endocrine therapy (ET) is a current standard first-/second-line treatment for hormone receptor (HR)-positive, HER2-negative advanced/metastatic breast cancer (AMBC). We aimed to provide real-world evidence regarding CDK4/6i therapy in this population.
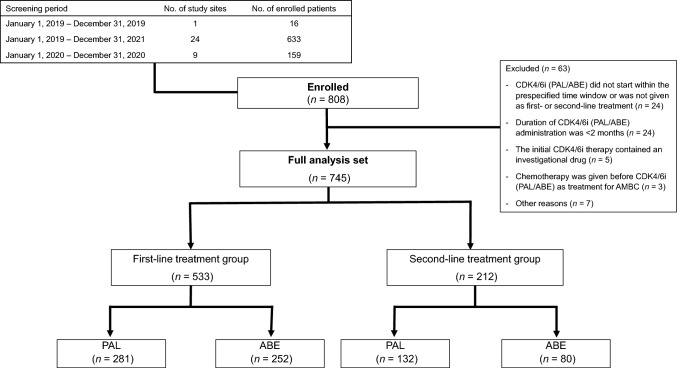
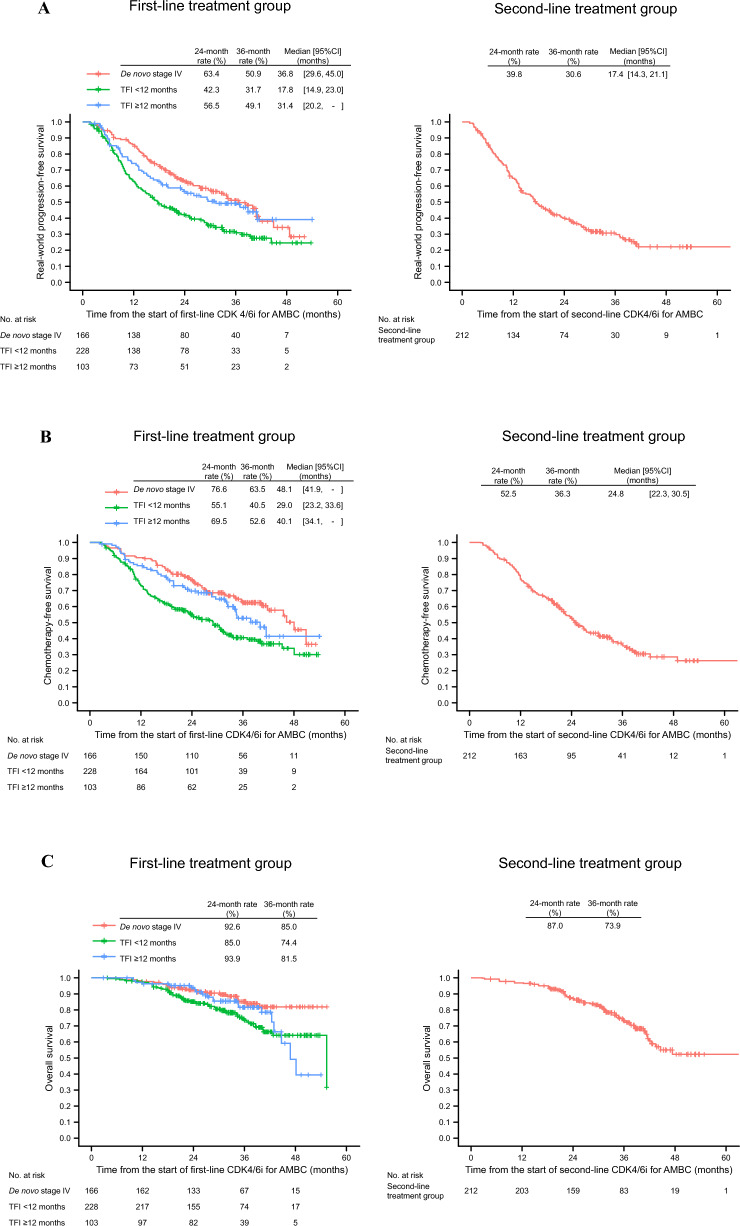
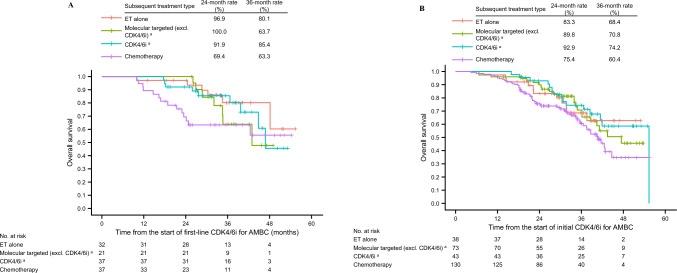
Methods: In this multicenter observational study, data from patients who had started CDK4/6i therapy between January 1, 2019, and December 31, 2021, as first-/second-line treatment for AMBC were used; real-world progression-free survival (rwPFS), chemotherapy-free survival, and overall survival were analyzed using the Kaplan-Meier method. Additionally, data were analyzed by separating patients with treatment-free interval (TFI) < 12 months (deemed resistant to ET) from the first-line treatment group (hereafter, the exclusive first-line treatment group).
Results: Data from 745 patients were analyzed. Compared with palbociclib, abemaciclib was used in younger patients and those with expected poor prognosis. Median rwPFS was 36.8, 17.8, and 31.4 months in patients with de novo stage IV disease, TFI < 12 months, and TFI ≥ 12 months, respectively, in the first-line treatment group, and 17.4 months in the second-line treatment group. In the exclusive first-line treatment group, median rwPFS of the subsequent treatment after initial CDK4/6i plus ET was < 7 months, regardless of the type of subsequent treatment; prognosis was especially poor in those who were switched to chemotherapy.
Conclusions: The real-world survival outcomes found in this study for patients receiving first-/second-line CDK4/6i therapy were consistent with those of randomized phase 3 studies. As outcomes of subsequent treatment after initial CDK4/6i plus ET remain insufficient, further improvement in treatment is necessary.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


