Chiara Milano, Pietro Businaro, Claudia Papi, Lionel Arlettaz, Laura Marmolejo, Laura Naranjo, Matteo Gastaldi, Raffaele Iorio, Albert Saiz, Jesús Planagumà, Esther Aguilar, Chiara Pizzanelli, Eugenia Martinez-Hernandez, Thaís Armangué, Mar Guasp, Raquel Ruiz-García, Lidia Sabater, Josep O Dalmau, Francesc Graus, Marianna Spatola
{"title":"评估自身免疫性神经系统疾病的商业组织检测(一):细胞内抗原抗体","authors":"Chiara Milano, Pietro Businaro, Claudia Papi, Lionel Arlettaz, Laura Marmolejo, Laura Naranjo, Matteo Gastaldi, Raffaele Iorio, Albert Saiz, Jesús Planagumà, Esther Aguilar, Chiara Pizzanelli, Eugenia Martinez-Hernandez, Thaís Armangué, Mar Guasp, Raquel Ruiz-García, Lidia Sabater, Josep O Dalmau, Francesc Graus, Marianna Spatola","doi":"10.1212/NXI.0000000000200410","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Current strategies to detect autoantibodies against intracellular neural antigens (IC-Abs) include tissue-based assays (TBAs) alongside line blots or cell-based assays (CBAs). Many clinical laboratories use commercially available TBAs as a screening test, but their diagnostic yield has not been assessed. We determined the performance of 2 commercial TBAs in detecting IC-Abs.</p><p><strong>Methods: </strong>We analyzed samples from 100 patients with autoimmune or paraneoplastic neurologic syndromes harboring IC-Abs (confirmed by in-house TBAs and line blots or CBAs) and 50 negative controls. IC-Abs samples included serum (10 each for Hu, Yo, Ri, SOX1, CV2, Ma2, Tr, amphiphysin, and GAD65 antibodies) or CSF (10 with GFAP antibodies) samples. Two commercial indirect immunofluorescence (IIF) TBAs (INOVA and EUROIMMUN) were assessed by 2 experienced investigators and 3 less experienced raters, all blinded to antibody status. Discordant results were re-evaluated through interrater discussion and assessed using Cohen's kappa.</p><p><strong>Results: </strong>The 2 experienced raters showed substantial agreement (85% for INOVA, 83% for EUROIMMUN) on negative/positive results, which increased to >95% after interrater discussion (Cohen's kappa 0.95 and 0.93, respectively). With IIF-INOVA, they correctly identified 118 of 150 samples (79%) and misclassified 28 of 150 (19%, 2 false positives and 26 false negatives) while results remained discordant in the remaining 4 of 150 samples (2%). With IIF-EUROIMMUN, they correctly identified 105 of 150 samples (70%) and misclassified 40 of 150 (27%, 6 false positives, 34 false negatives), with discordance in 5 of 150 samples (3%). Overall, the sensitivity was 73% for IIF-INOVA and 66% for IIF-EUROIMMUN. The specificity was 96% for IIF-INOVA and 88% for IIF-EUROIMMUN. Both TBAs showed low sensitivity in detecting CV2, SOX1, and amphiphysin antibodies while Ma2 antibodies were missed mainly by IIF-EUROIMMUN and Hu/Ri antibodies by IIF-INOVA. Antibody-specific immunostaining patterns were correctly identified in 62 of 100 positive samples with IIF-INOVA and 55 of 100 with IIF-EUROIMMUN (<i>p</i> = 0.34). Less experienced raters showed higher rates of false-positive results (up to 22% with IIF-EUROIMMUN).</p><p><strong>Discussion: </strong>The performance of commercial IIF-TBAs for IC-Abs detection is suboptimal, exhibiting high false-negative rates of 25%-35%. Therefore, commercial TBAs should not be used alone for IC-Abs screening, but alongside more sensitive techniques, such as line blots. Discordant results between 2 techniques should prompt retesting in reference centers with in-house TBAs, particularly when the suspicion of an autoimmune or paraneoplastic syndrome is high.</p>","PeriodicalId":19472,"journal":{"name":"Neurology® Neuroimmunology & Neuroinflammation","volume":"12 4","pages":"e200410"},"PeriodicalIF":7.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12153943/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessing Commercial Tissue-Based Assays for Autoimmune Neurologic Disorders (I): Antibodies to Intracellular Antigens.\",\"authors\":\"Chiara Milano, Pietro Businaro, Claudia Papi, Lionel Arlettaz, Laura Marmolejo, Laura Naranjo, Matteo Gastaldi, Raffaele Iorio, Albert Saiz, Jesús Planagumà, Esther Aguilar, Chiara Pizzanelli, Eugenia Martinez-Hernandez, Thaís Armangué, Mar Guasp, Raquel Ruiz-García, Lidia Sabater, Josep O Dalmau, Francesc Graus, Marianna Spatola\",\"doi\":\"10.1212/NXI.0000000000200410\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Current strategies to detect autoantibodies against intracellular neural antigens (IC-Abs) include tissue-based assays (TBAs) alongside line blots or cell-based assays (CBAs). Many clinical laboratories use commercially available TBAs as a screening test, but their diagnostic yield has not been assessed. We determined the performance of 2 commercial TBAs in detecting IC-Abs.</p><p><strong>Methods: </strong>We analyzed samples from 100 patients with autoimmune or paraneoplastic neurologic syndromes harboring IC-Abs (confirmed by in-house TBAs and line blots or CBAs) and 50 negative controls. IC-Abs samples included serum (10 each for Hu, Yo, Ri, SOX1, CV2, Ma2, Tr, amphiphysin, and GAD65 antibodies) or CSF (10 with GFAP antibodies) samples. Two commercial indirect immunofluorescence (IIF) TBAs (INOVA and EUROIMMUN) were assessed by 2 experienced investigators and 3 less experienced raters, all blinded to antibody status. Discordant results were re-evaluated through interrater discussion and assessed using Cohen's kappa.</p><p><strong>Results: </strong>The 2 experienced raters showed substantial agreement (85% for INOVA, 83% for EUROIMMUN) on negative/positive results, which increased to >95% after interrater discussion (Cohen's kappa 0.95 and 0.93, respectively). With IIF-INOVA, they correctly identified 118 of 150 samples (79%) and misclassified 28 of 150 (19%, 2 false positives and 26 false negatives) while results remained discordant in the remaining 4 of 150 samples (2%). With IIF-EUROIMMUN, they correctly identified 105 of 150 samples (70%) and misclassified 40 of 150 (27%, 6 false positives, 34 false negatives), with discordance in 5 of 150 samples (3%). Overall, the sensitivity was 73% for IIF-INOVA and 66% for IIF-EUROIMMUN. The specificity was 96% for IIF-INOVA and 88% for IIF-EUROIMMUN. Both TBAs showed low sensitivity in detecting CV2, SOX1, and amphiphysin antibodies while Ma2 antibodies were missed mainly by IIF-EUROIMMUN and Hu/Ri antibodies by IIF-INOVA. Antibody-specific immunostaining patterns were correctly identified in 62 of 100 positive samples with IIF-INOVA and 55 of 100 with IIF-EUROIMMUN (<i>p</i> = 0.34). Less experienced raters showed higher rates of false-positive results (up to 22% with IIF-EUROIMMUN).</p><p><strong>Discussion: </strong>The performance of commercial IIF-TBAs for IC-Abs detection is suboptimal, exhibiting high false-negative rates of 25%-35%. Therefore, commercial TBAs should not be used alone for IC-Abs screening, but alongside more sensitive techniques, such as line blots. Discordant results between 2 techniques should prompt retesting in reference centers with in-house TBAs, particularly when the suspicion of an autoimmune or paraneoplastic syndrome is high.</p>\",\"PeriodicalId\":19472,\"journal\":{\"name\":\"Neurology® Neuroimmunology & Neuroinflammation\",\"volume\":\"12 4\",\"pages\":\"e200410\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12153943/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology® Neuroimmunology & Neuroinflammation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1212/NXI.0000000000200410\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology® Neuroimmunology & Neuroinflammation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000200410","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/20 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Assessing Commercial Tissue-Based Assays for Autoimmune Neurologic Disorders (I): Antibodies to Intracellular Antigens.
Background and objectives: Current strategies to detect autoantibodies against intracellular neural antigens (IC-Abs) include tissue-based assays (TBAs) alongside line blots or cell-based assays (CBAs). Many clinical laboratories use commercially available TBAs as a screening test, but their diagnostic yield has not been assessed. We determined the performance of 2 commercial TBAs in detecting IC-Abs.
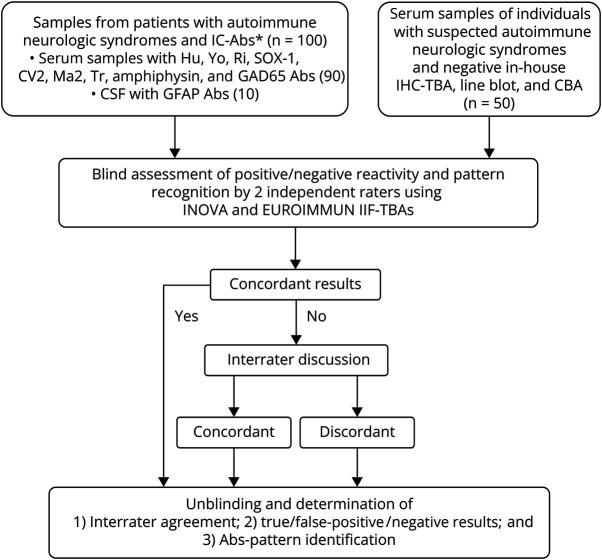
Methods: We analyzed samples from 100 patients with autoimmune or paraneoplastic neurologic syndromes harboring IC-Abs (confirmed by in-house TBAs and line blots or CBAs) and 50 negative controls. IC-Abs samples included serum (10 each for Hu, Yo, Ri, SOX1, CV2, Ma2, Tr, amphiphysin, and GAD65 antibodies) or CSF (10 with GFAP antibodies) samples. Two commercial indirect immunofluorescence (IIF) TBAs (INOVA and EUROIMMUN) were assessed by 2 experienced investigators and 3 less experienced raters, all blinded to antibody status. Discordant results were re-evaluated through interrater discussion and assessed using Cohen's kappa.
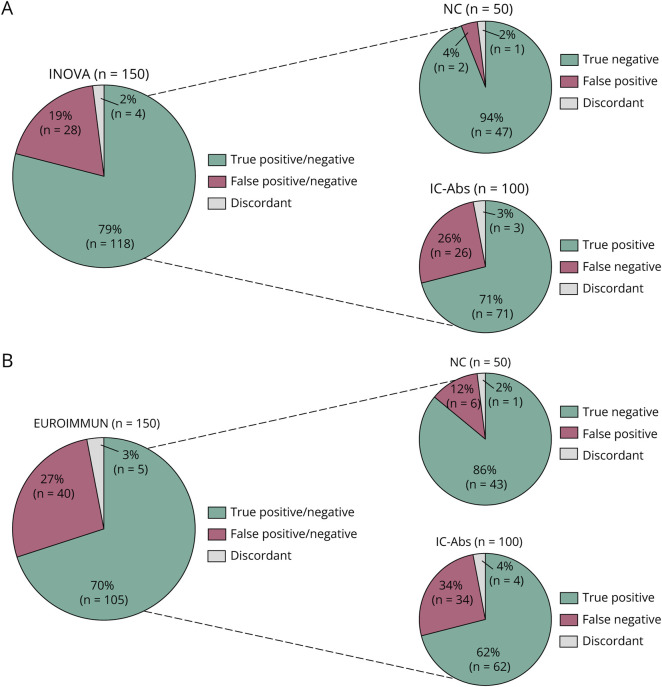
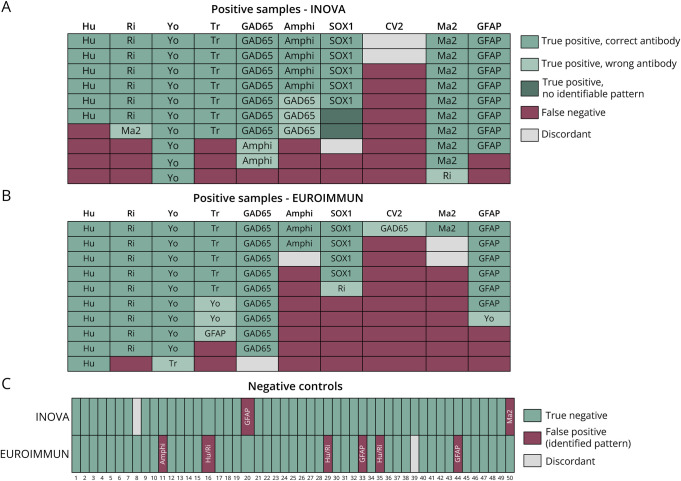
Results: The 2 experienced raters showed substantial agreement (85% for INOVA, 83% for EUROIMMUN) on negative/positive results, which increased to >95% after interrater discussion (Cohen's kappa 0.95 and 0.93, respectively). With IIF-INOVA, they correctly identified 118 of 150 samples (79%) and misclassified 28 of 150 (19%, 2 false positives and 26 false negatives) while results remained discordant in the remaining 4 of 150 samples (2%). With IIF-EUROIMMUN, they correctly identified 105 of 150 samples (70%) and misclassified 40 of 150 (27%, 6 false positives, 34 false negatives), with discordance in 5 of 150 samples (3%). Overall, the sensitivity was 73% for IIF-INOVA and 66% for IIF-EUROIMMUN. The specificity was 96% for IIF-INOVA and 88% for IIF-EUROIMMUN. Both TBAs showed low sensitivity in detecting CV2, SOX1, and amphiphysin antibodies while Ma2 antibodies were missed mainly by IIF-EUROIMMUN and Hu/Ri antibodies by IIF-INOVA. Antibody-specific immunostaining patterns were correctly identified in 62 of 100 positive samples with IIF-INOVA and 55 of 100 with IIF-EUROIMMUN (p = 0.34). Less experienced raters showed higher rates of false-positive results (up to 22% with IIF-EUROIMMUN).
Discussion: The performance of commercial IIF-TBAs for IC-Abs detection is suboptimal, exhibiting high false-negative rates of 25%-35%. Therefore, commercial TBAs should not be used alone for IC-Abs screening, but alongside more sensitive techniques, such as line blots. Discordant results between 2 techniques should prompt retesting in reference centers with in-house TBAs, particularly when the suspicion of an autoimmune or paraneoplastic syndrome is high.
期刊介绍:
Neurology Neuroimmunology & Neuroinflammation is an official journal of the American Academy of Neurology. Neurology: Neuroimmunology & Neuroinflammation will be the premier peer-reviewed journal in neuroimmunology and neuroinflammation. This journal publishes rigorously peer-reviewed open-access reports of original research and in-depth reviews of topics in neuroimmunology & neuroinflammation, affecting the full range of neurologic diseases including (but not limited to) Alzheimer's disease, Parkinson's disease, ALS, tauopathy, and stroke; multiple sclerosis and NMO; inflammatory peripheral nerve and muscle disease, Guillain-Barré and myasthenia gravis; nervous system infection; paraneoplastic syndromes, noninfectious encephalitides and other antibody-mediated disorders; and psychiatric and neurodevelopmental disorders. Clinical trials, instructive case reports, and small case series will also be featured.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


