Lauren Bosley, Clinton Gibbs, Eunah Joo, Geoffrey Dobson
{"title":"非神经外科医生可以在非大都市地区进行创伤性脑损伤手术吗?范围检讨","authors":"Lauren Bosley, Clinton Gibbs, Eunah Joo, Geoffrey Dobson","doi":"10.1111/1742-6723.70055","DOIUrl":null,"url":null,"abstract":"<p>Traumatic brain injuries (TBIs) with increased intracranial pressure (ICP) require time-sensitive surgical intervention. In non-metropolitan areas, neurosurgeons are often unavailable to provide definitive treatment. Therapeutic surgical intervention by a non-neurosurgeon, for example, general surgeons, is a potential alternative; however, the feasibility and utility of non-specialist intervention are poorly defined within the literature. A scoping review was conducted within Scopus, Emcare, MEDLINE and CINAHL for original literature about emergency neurosurgical interventions performed by a non-neurosurgeon for TBIs in non-metropolitan settings without prompt access to a neurosurgeon. This search yielded 20 studies that included over 2000 surgical interventions in 13 countries. General surgeons most commonly performed the procedures on patients with computed tomography (CT)-confirmed lesions. Mortality rates were heterogeneous, ranging from 0% to 67% in small cohorts with variable follow-up periods. Mortality was consistently higher in patients with subdural haematomas (SDHs) opposed to extradural haematomas (EDHs). Morbidity was measured in 13 studies, commonly via the Glasgow outcome scale (GOS). Most studies had access to remote neurosurgical advice via telehealth. Overall, these 20 studies provided incomplete information regarding mortality rates and functional outcomes from this alternative practise. The present study concludes that emergency decompression by a non-neurosurgeon for patients with severe TBIs may be lifesaving for patients without timely access to a neurosurgical centre. Our study further highlights the need for further research, training and resource allocation, including strengthening telecommunication pathways, to support patient access to lifesaving neurosurgical interventions in these environments, and ultimately address surgical inequalities in rural and remote regions of the world.</p>","PeriodicalId":11604,"journal":{"name":"Emergency Medicine Australasia","volume":"37 3","pages":""},"PeriodicalIF":1.4000,"publicationDate":"2025-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1742-6723.70055","citationCount":"0","resultStr":"{\"title\":\"Can Non-Neurosurgeons Operate on Traumatic Brain Injuries in Non-Metropolitan Areas? A Scoping Review\",\"authors\":\"Lauren Bosley, Clinton Gibbs, Eunah Joo, Geoffrey Dobson\",\"doi\":\"10.1111/1742-6723.70055\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Traumatic brain injuries (TBIs) with increased intracranial pressure (ICP) require time-sensitive surgical intervention. In non-metropolitan areas, neurosurgeons are often unavailable to provide definitive treatment. Therapeutic surgical intervention by a non-neurosurgeon, for example, general surgeons, is a potential alternative; however, the feasibility and utility of non-specialist intervention are poorly defined within the literature. A scoping review was conducted within Scopus, Emcare, MEDLINE and CINAHL for original literature about emergency neurosurgical interventions performed by a non-neurosurgeon for TBIs in non-metropolitan settings without prompt access to a neurosurgeon. This search yielded 20 studies that included over 2000 surgical interventions in 13 countries. General surgeons most commonly performed the procedures on patients with computed tomography (CT)-confirmed lesions. Mortality rates were heterogeneous, ranging from 0% to 67% in small cohorts with variable follow-up periods. Mortality was consistently higher in patients with subdural haematomas (SDHs) opposed to extradural haematomas (EDHs). Morbidity was measured in 13 studies, commonly via the Glasgow outcome scale (GOS). Most studies had access to remote neurosurgical advice via telehealth. Overall, these 20 studies provided incomplete information regarding mortality rates and functional outcomes from this alternative practise. The present study concludes that emergency decompression by a non-neurosurgeon for patients with severe TBIs may be lifesaving for patients without timely access to a neurosurgical centre. Our study further highlights the need for further research, training and resource allocation, including strengthening telecommunication pathways, to support patient access to lifesaving neurosurgical interventions in these environments, and ultimately address surgical inequalities in rural and remote regions of the world.</p>\",\"PeriodicalId\":11604,\"journal\":{\"name\":\"Emergency Medicine Australasia\",\"volume\":\"37 3\",\"pages\":\"\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2025-05-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1742-6723.70055\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Emergency Medicine Australasia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/1742-6723.70055\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emergency Medicine Australasia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1742-6723.70055","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Can Non-Neurosurgeons Operate on Traumatic Brain Injuries in Non-Metropolitan Areas? A Scoping Review
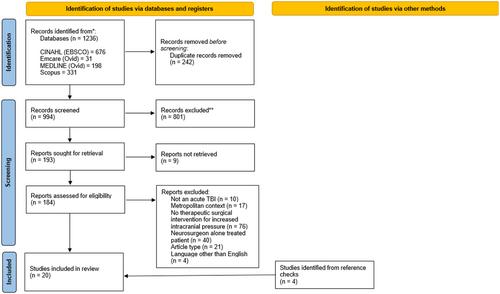
Traumatic brain injuries (TBIs) with increased intracranial pressure (ICP) require time-sensitive surgical intervention. In non-metropolitan areas, neurosurgeons are often unavailable to provide definitive treatment. Therapeutic surgical intervention by a non-neurosurgeon, for example, general surgeons, is a potential alternative; however, the feasibility and utility of non-specialist intervention are poorly defined within the literature. A scoping review was conducted within Scopus, Emcare, MEDLINE and CINAHL for original literature about emergency neurosurgical interventions performed by a non-neurosurgeon for TBIs in non-metropolitan settings without prompt access to a neurosurgeon. This search yielded 20 studies that included over 2000 surgical interventions in 13 countries. General surgeons most commonly performed the procedures on patients with computed tomography (CT)-confirmed lesions. Mortality rates were heterogeneous, ranging from 0% to 67% in small cohorts with variable follow-up periods. Mortality was consistently higher in patients with subdural haematomas (SDHs) opposed to extradural haematomas (EDHs). Morbidity was measured in 13 studies, commonly via the Glasgow outcome scale (GOS). Most studies had access to remote neurosurgical advice via telehealth. Overall, these 20 studies provided incomplete information regarding mortality rates and functional outcomes from this alternative practise. The present study concludes that emergency decompression by a non-neurosurgeon for patients with severe TBIs may be lifesaving for patients without timely access to a neurosurgical centre. Our study further highlights the need for further research, training and resource allocation, including strengthening telecommunication pathways, to support patient access to lifesaving neurosurgical interventions in these environments, and ultimately address surgical inequalities in rural and remote regions of the world.
期刊介绍:
Emergency Medicine Australasia is the official journal of the Australasian College for Emergency Medicine (ACEM) and the Australasian Society for Emergency Medicine (ASEM), and publishes original articles dealing with all aspects of clinical practice, research, education and experiences in emergency medicine.
Original articles are published under the following sections: Original Research, Paediatric Emergency Medicine, Disaster Medicine, Education and Training, Ethics, International Emergency Medicine, Management and Quality, Medicolegal Matters, Prehospital Care, Public Health, Rural and Remote Care, Technology, Toxicology and Trauma. Accepted papers become the copyright of the journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


