Sonia Martinez Alcaide , Izaskun Balciscueta Coltell , Ricardo Bou Monterde , Maria Jose Enguix Soriano , Pedro Juan Gonzalez Noguera , Francisco Javier Del Pino Porres
{"title":"乳腺癌原发性全身治疗后肿瘤完全缓解的预测因素分析。","authors":"Sonia Martinez Alcaide , Izaskun Balciscueta Coltell , Ricardo Bou Monterde , Maria Jose Enguix Soriano , Pedro Juan Gonzalez Noguera , Francisco Javier Del Pino Porres","doi":"10.1016/j.cireng.2025.800112","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><div>Primary systemic therapy in breast cancer is an effective tool for increasing pathological complete response prior to surgery and improving patient survival. The main objective of this study was to analyze the predictive variables for complete tumor response after neoadjuvant therapy.</div></div><div><h3>Methods</h3><div>Data from 146 breast cancer patients treated with primary systemic therapy at La Ribera Hospital between 2018 and 2022 were reviewed. Statistical methods were employed using SPSS 23 software to identify factors predicting tumor response to treatment.</div></div><div><h3>Results</h3><div>Among the patients analyzed, 22.6% presented complete response according to magnetic resonance imaging, and 31.5% showed no residual tumor in the surgical specimen. In the univariate analysis, variables associated with higher presence of residual tumor included lymphovascular invasion (<em>P</em> = 0; 95%CI: 2.361−45.390), luminal B subtype (<em>P</em> = .039; 95%CI: 1.028−5.826), and sentinel node involvement or positive axillary nodes in axillary lymphadenectomy (<em>P</em> = .031; 95%CI: 1.006−72.361). Conversely, tumors smaller than 2 cm (<em>P</em> = .002; 95%CI: 1.567−7.535) and the Her2+ subtype (<em>P</em> = .004; 95%CI: 0.086−0.667) were associated with a higher likelihood of no residual tumor. In the multivariate analysis, lymphovascular invasion was the only statistically significant factor associated with the presence of residual tumor (<em>P</em> = .021; 95%CI: 0.037−0.760).</div></div><div><h3>Conclusions</h3><div>Lymphovascular invasion was identified as a predictor of lack of response to neoadjuvant treatment. Additionally, the Her2+ subtype demonstrated the best response to preoperative therapy. These findings suggest that, to improve therapeutic outcomes, it is crucial to consider these variables when personalizing patient treatment.</div></div>","PeriodicalId":93935,"journal":{"name":"Cirugia espanola","volume":"103 7","pages":"Article 800112"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Analysis of predictors for complete tumor response after primary systemic therapy in breast cancer\",\"authors\":\"Sonia Martinez Alcaide , Izaskun Balciscueta Coltell , Ricardo Bou Monterde , Maria Jose Enguix Soriano , Pedro Juan Gonzalez Noguera , Francisco Javier Del Pino Porres\",\"doi\":\"10.1016/j.cireng.2025.800112\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Introduction</h3><div>Primary systemic therapy in breast cancer is an effective tool for increasing pathological complete response prior to surgery and improving patient survival. The main objective of this study was to analyze the predictive variables for complete tumor response after neoadjuvant therapy.</div></div><div><h3>Methods</h3><div>Data from 146 breast cancer patients treated with primary systemic therapy at La Ribera Hospital between 2018 and 2022 were reviewed. Statistical methods were employed using SPSS 23 software to identify factors predicting tumor response to treatment.</div></div><div><h3>Results</h3><div>Among the patients analyzed, 22.6% presented complete response according to magnetic resonance imaging, and 31.5% showed no residual tumor in the surgical specimen. In the univariate analysis, variables associated with higher presence of residual tumor included lymphovascular invasion (<em>P</em> = 0; 95%CI: 2.361−45.390), luminal B subtype (<em>P</em> = .039; 95%CI: 1.028−5.826), and sentinel node involvement or positive axillary nodes in axillary lymphadenectomy (<em>P</em> = .031; 95%CI: 1.006−72.361). Conversely, tumors smaller than 2 cm (<em>P</em> = .002; 95%CI: 1.567−7.535) and the Her2+ subtype (<em>P</em> = .004; 95%CI: 0.086−0.667) were associated with a higher likelihood of no residual tumor. In the multivariate analysis, lymphovascular invasion was the only statistically significant factor associated with the presence of residual tumor (<em>P</em> = .021; 95%CI: 0.037−0.760).</div></div><div><h3>Conclusions</h3><div>Lymphovascular invasion was identified as a predictor of lack of response to neoadjuvant treatment. Additionally, the Her2+ subtype demonstrated the best response to preoperative therapy. These findings suggest that, to improve therapeutic outcomes, it is crucial to consider these variables when personalizing patient treatment.</div></div>\",\"PeriodicalId\":93935,\"journal\":{\"name\":\"Cirugia espanola\",\"volume\":\"103 7\",\"pages\":\"Article 800112\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cirugia espanola\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2173507725000754\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cirugia espanola","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2173507725000754","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Analysis of predictors for complete tumor response after primary systemic therapy in breast cancer
Introduction
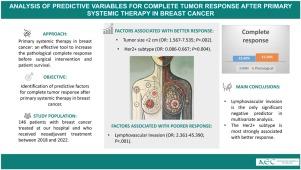
Primary systemic therapy in breast cancer is an effective tool for increasing pathological complete response prior to surgery and improving patient survival. The main objective of this study was to analyze the predictive variables for complete tumor response after neoadjuvant therapy.
Methods
Data from 146 breast cancer patients treated with primary systemic therapy at La Ribera Hospital between 2018 and 2022 were reviewed. Statistical methods were employed using SPSS 23 software to identify factors predicting tumor response to treatment.
Results
Among the patients analyzed, 22.6% presented complete response according to magnetic resonance imaging, and 31.5% showed no residual tumor in the surgical specimen. In the univariate analysis, variables associated with higher presence of residual tumor included lymphovascular invasion (P = 0; 95%CI: 2.361−45.390), luminal B subtype (P = .039; 95%CI: 1.028−5.826), and sentinel node involvement or positive axillary nodes in axillary lymphadenectomy (P = .031; 95%CI: 1.006−72.361). Conversely, tumors smaller than 2 cm (P = .002; 95%CI: 1.567−7.535) and the Her2+ subtype (P = .004; 95%CI: 0.086−0.667) were associated with a higher likelihood of no residual tumor. In the multivariate analysis, lymphovascular invasion was the only statistically significant factor associated with the presence of residual tumor (P = .021; 95%CI: 0.037−0.760).
Conclusions
Lymphovascular invasion was identified as a predictor of lack of response to neoadjuvant treatment. Additionally, the Her2+ subtype demonstrated the best response to preoperative therapy. These findings suggest that, to improve therapeutic outcomes, it is crucial to consider these variables when personalizing patient treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


