{"title":"入住重症监护室的间质性肺疾病加重的管理策略和预后预测因素:一项叙述性回顾","authors":"Ans Alamami","doi":"10.2478/jccm-2025-0013","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Interstitial lung disease (ILD) is a cluster of diseases that affect the lungs, characterized by different degrees of inflammation and fibrosis within the parenchyma. In the intensive care unit (ICU), ILD poses substantial challenges because of its complicated nature and high morbidity and mortality rates in severe cases. ILD pathophysiology frequently entails persistent inflammation that results in fibrosis, disrupting the typical structure and function of the lung. Patients with ILD frequently experience dyspnea, non-productive cough, and tiredness. In the ICU setting, these symptoms may worsen and lead to signs of acute respiratory failure with significantly impaired gas physiology.</p><p><strong>Methodology: </strong>A systematic search was conducted in reputable databases, including PubMed, Google Scholar, and Embase. To ensure a comprehensive search, a combination of keywords such as \"interstitial lung disease,\" \"intensive care,\" and \"outcomes\" was used. Studies published within the last ten years reporting on the outcomes of ILD patients admitted to intensive care included.</p><p><strong>Result: </strong>Effective management of ILD in an ICU setting is challenging and requires a comprehensive approach to address the triggering factor and providing respiratory support, Hypoxemia severity is a critical predictor of mortality, with lower PaO<sub>2</sub>/FiO<sub>2</sub> ratios during the first three days of ICU admission associated with increased mortality rates. The need for mechanical ventilation, particularly invasive mechanical ventilation (IMV), is a significant predictor of poor outcomes in ILD patients. Additionally, higher positive end-expiratory pressure (PEEP) settings, and severity of illness scores, such as the Acute Physiology and Chronic Health Evaluation (APACHE) score, are also linked to increased mortality. Other poor prognostic factors include the presence of shock and pulmonary fibrosis on computed tomography (CT) images. Among the various types of ILDs, idiopathic pulmonary fibrosis (IPF) is associated with the highest mortality rate. Furthermore, a high ventilatory ratio (VR) within 24 hours after intubation independently predicts ICU mortality.</p><p><strong>Conclusion: </strong>This literature review points out outcome predictors of interstitial lung disease in intensive care units, which are mainly hypoxemia, the severity of the illness, invasive ventilation, the presence of shock, and the extent of fibrosis on CT Images.</p>","PeriodicalId":44227,"journal":{"name":"Journal of Critical Care Medicine","volume":"11 2","pages":"112-121"},"PeriodicalIF":1.7000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12080564/pdf/","citationCount":"0","resultStr":"{\"title\":\"Management strategies and outcomes predictors of interstitial lung disease exacerbation admitted to an intensive care setting: A narrative review.\",\"authors\":\"Ans Alamami\",\"doi\":\"10.2478/jccm-2025-0013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Interstitial lung disease (ILD) is a cluster of diseases that affect the lungs, characterized by different degrees of inflammation and fibrosis within the parenchyma. In the intensive care unit (ICU), ILD poses substantial challenges because of its complicated nature and high morbidity and mortality rates in severe cases. ILD pathophysiology frequently entails persistent inflammation that results in fibrosis, disrupting the typical structure and function of the lung. Patients with ILD frequently experience dyspnea, non-productive cough, and tiredness. In the ICU setting, these symptoms may worsen and lead to signs of acute respiratory failure with significantly impaired gas physiology.</p><p><strong>Methodology: </strong>A systematic search was conducted in reputable databases, including PubMed, Google Scholar, and Embase. To ensure a comprehensive search, a combination of keywords such as \\\"interstitial lung disease,\\\" \\\"intensive care,\\\" and \\\"outcomes\\\" was used. Studies published within the last ten years reporting on the outcomes of ILD patients admitted to intensive care included.</p><p><strong>Result: </strong>Effective management of ILD in an ICU setting is challenging and requires a comprehensive approach to address the triggering factor and providing respiratory support, Hypoxemia severity is a critical predictor of mortality, with lower PaO<sub>2</sub>/FiO<sub>2</sub> ratios during the first three days of ICU admission associated with increased mortality rates. The need for mechanical ventilation, particularly invasive mechanical ventilation (IMV), is a significant predictor of poor outcomes in ILD patients. Additionally, higher positive end-expiratory pressure (PEEP) settings, and severity of illness scores, such as the Acute Physiology and Chronic Health Evaluation (APACHE) score, are also linked to increased mortality. Other poor prognostic factors include the presence of shock and pulmonary fibrosis on computed tomography (CT) images. Among the various types of ILDs, idiopathic pulmonary fibrosis (IPF) is associated with the highest mortality rate. Furthermore, a high ventilatory ratio (VR) within 24 hours after intubation independently predicts ICU mortality.</p><p><strong>Conclusion: </strong>This literature review points out outcome predictors of interstitial lung disease in intensive care units, which are mainly hypoxemia, the severity of the illness, invasive ventilation, the presence of shock, and the extent of fibrosis on CT Images.</p>\",\"PeriodicalId\":44227,\"journal\":{\"name\":\"Journal of Critical Care Medicine\",\"volume\":\"11 2\",\"pages\":\"112-121\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12080564/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Critical Care Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2478/jccm-2025-0013\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Critical Care Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2478/jccm-2025-0013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Management strategies and outcomes predictors of interstitial lung disease exacerbation admitted to an intensive care setting: A narrative review.
Background: Interstitial lung disease (ILD) is a cluster of diseases that affect the lungs, characterized by different degrees of inflammation and fibrosis within the parenchyma. In the intensive care unit (ICU), ILD poses substantial challenges because of its complicated nature and high morbidity and mortality rates in severe cases. ILD pathophysiology frequently entails persistent inflammation that results in fibrosis, disrupting the typical structure and function of the lung. Patients with ILD frequently experience dyspnea, non-productive cough, and tiredness. In the ICU setting, these symptoms may worsen and lead to signs of acute respiratory failure with significantly impaired gas physiology.
Methodology: A systematic search was conducted in reputable databases, including PubMed, Google Scholar, and Embase. To ensure a comprehensive search, a combination of keywords such as "interstitial lung disease," "intensive care," and "outcomes" was used. Studies published within the last ten years reporting on the outcomes of ILD patients admitted to intensive care included.
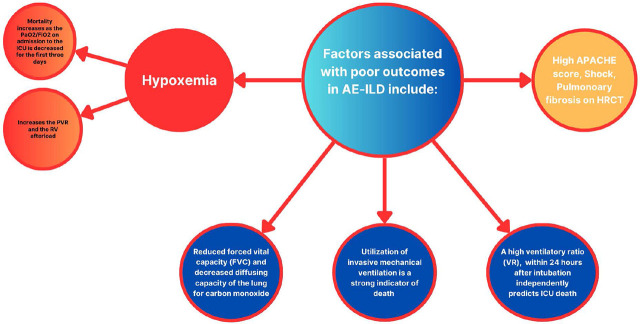
Result: Effective management of ILD in an ICU setting is challenging and requires a comprehensive approach to address the triggering factor and providing respiratory support, Hypoxemia severity is a critical predictor of mortality, with lower PaO2/FiO2 ratios during the first three days of ICU admission associated with increased mortality rates. The need for mechanical ventilation, particularly invasive mechanical ventilation (IMV), is a significant predictor of poor outcomes in ILD patients. Additionally, higher positive end-expiratory pressure (PEEP) settings, and severity of illness scores, such as the Acute Physiology and Chronic Health Evaluation (APACHE) score, are also linked to increased mortality. Other poor prognostic factors include the presence of shock and pulmonary fibrosis on computed tomography (CT) images. Among the various types of ILDs, idiopathic pulmonary fibrosis (IPF) is associated with the highest mortality rate. Furthermore, a high ventilatory ratio (VR) within 24 hours after intubation independently predicts ICU mortality.
Conclusion: This literature review points out outcome predictors of interstitial lung disease in intensive care units, which are mainly hypoxemia, the severity of the illness, invasive ventilation, the presence of shock, and the extent of fibrosis on CT Images.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


