Mary E Horner, Alexis Ogdie, Kate K Orroth, Shia T Kent, Kathy V Tran, Cynthia Deignan, Myriam Cordey, M Alan Brookhart
{"title":"实施阴性对照结果评估银屑病和银屑病关节炎治疗的可比性。","authors":"Mary E Horner, Alexis Ogdie, Kate K Orroth, Shia T Kent, Kathy V Tran, Cynthia Deignan, Myriam Cordey, M Alan Brookhart","doi":"10.1002/pds.70156","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Treatment selection is typically associated with prognosis, leading to potential confounding in comparative studies. We used negative control outcomes (NCOs) to identify potential residual confounding when comparing apremilast initiators to other psoriasis (PsO) or psoriatic arthritis (PsA) treatment initiators.</p><p><strong>Methods: </strong>Adults with PsO/PsA who initiated treatment from September 23/March 21, 2016, respectively, with apremilast, topicals, methotrexate, interleukin (IL)-17 inhibitor (i), IL-12/23i, or tumor necrosis factor inhibitor (TNFi) were identified in the OPTUM Clinformatics DataMart database. Follow-up ended at treatment switch/discontinuation, NCO, end of enrollment, or September 30, 2022. NCOs addressed confounding for healthy users (wellness visit, herpes zoster vaccine, colon cancer screening, pelvic screening), functional status (accidents), and channeling. The 1-year relative risk (RR) for each NCO was estimated for all treatment comparisons using an inverse probability of treatment and censoring weighted estimator.</p><p><strong>Results: </strong>In PsO, potential healthy user bias was detected in apremilast vs. IL-17i initiators, with a higher likelihood of herpes zoster vaccine and colon cancer screening (RR [95% CI]: 2.01 [1.41, 2.88] and 1.42 [1.13, 1.77], respectively). Wellness visits and pelvic exams were less likely among apremilast vs. topical initiators (0.84 [0.72, 0.98] and 0.83 [0.70, 0.98], respectively). The wellness visit RR was attenuated in individuals with ≥ 1 pre-index topical prescription (0.90 [0.78, 1.04]). In PsA, minimal residual confounding was observed between apremilast and other treatments.</p><p><strong>Conclusions: </strong>Eligibility criteria (prior topicals) and weighting reduced residual confounding when comparing apremilast vs. other treatments for PsO and PsA. Integration of NCOs into comparative effectiveness/safety studies of PsO/PsA treatments may help identify unmeasured confounding.</p>","PeriodicalId":19782,"journal":{"name":"Pharmacoepidemiology and Drug Safety","volume":"34 5","pages":"e70156"},"PeriodicalIF":2.4000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12087269/pdf/","citationCount":"0","resultStr":"{\"title\":\"Implementing Negative Control Outcomes to Assess Comparability of Treatments for Psoriasis and Psoriatic Arthritis.\",\"authors\":\"Mary E Horner, Alexis Ogdie, Kate K Orroth, Shia T Kent, Kathy V Tran, Cynthia Deignan, Myriam Cordey, M Alan Brookhart\",\"doi\":\"10.1002/pds.70156\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Treatment selection is typically associated with prognosis, leading to potential confounding in comparative studies. We used negative control outcomes (NCOs) to identify potential residual confounding when comparing apremilast initiators to other psoriasis (PsO) or psoriatic arthritis (PsA) treatment initiators.</p><p><strong>Methods: </strong>Adults with PsO/PsA who initiated treatment from September 23/March 21, 2016, respectively, with apremilast, topicals, methotrexate, interleukin (IL)-17 inhibitor (i), IL-12/23i, or tumor necrosis factor inhibitor (TNFi) were identified in the OPTUM Clinformatics DataMart database. Follow-up ended at treatment switch/discontinuation, NCO, end of enrollment, or September 30, 2022. NCOs addressed confounding for healthy users (wellness visit, herpes zoster vaccine, colon cancer screening, pelvic screening), functional status (accidents), and channeling. The 1-year relative risk (RR) for each NCO was estimated for all treatment comparisons using an inverse probability of treatment and censoring weighted estimator.</p><p><strong>Results: </strong>In PsO, potential healthy user bias was detected in apremilast vs. IL-17i initiators, with a higher likelihood of herpes zoster vaccine and colon cancer screening (RR [95% CI]: 2.01 [1.41, 2.88] and 1.42 [1.13, 1.77], respectively). Wellness visits and pelvic exams were less likely among apremilast vs. topical initiators (0.84 [0.72, 0.98] and 0.83 [0.70, 0.98], respectively). The wellness visit RR was attenuated in individuals with ≥ 1 pre-index topical prescription (0.90 [0.78, 1.04]). In PsA, minimal residual confounding was observed between apremilast and other treatments.</p><p><strong>Conclusions: </strong>Eligibility criteria (prior topicals) and weighting reduced residual confounding when comparing apremilast vs. other treatments for PsO and PsA. Integration of NCOs into comparative effectiveness/safety studies of PsO/PsA treatments may help identify unmeasured confounding.</p>\",\"PeriodicalId\":19782,\"journal\":{\"name\":\"Pharmacoepidemiology and Drug Safety\",\"volume\":\"34 5\",\"pages\":\"e70156\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12087269/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pharmacoepidemiology and Drug Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/pds.70156\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacoepidemiology and Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pds.70156","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Implementing Negative Control Outcomes to Assess Comparability of Treatments for Psoriasis and Psoriatic Arthritis.
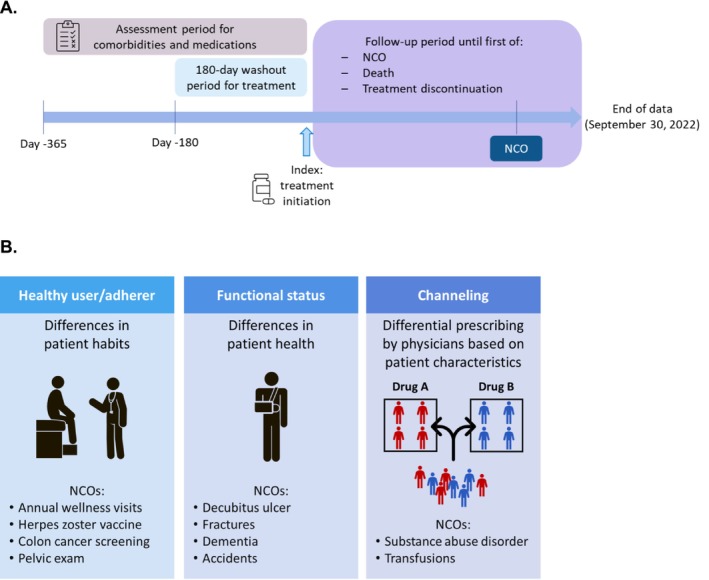
Purpose: Treatment selection is typically associated with prognosis, leading to potential confounding in comparative studies. We used negative control outcomes (NCOs) to identify potential residual confounding when comparing apremilast initiators to other psoriasis (PsO) or psoriatic arthritis (PsA) treatment initiators.
Methods: Adults with PsO/PsA who initiated treatment from September 23/March 21, 2016, respectively, with apremilast, topicals, methotrexate, interleukin (IL)-17 inhibitor (i), IL-12/23i, or tumor necrosis factor inhibitor (TNFi) were identified in the OPTUM Clinformatics DataMart database. Follow-up ended at treatment switch/discontinuation, NCO, end of enrollment, or September 30, 2022. NCOs addressed confounding for healthy users (wellness visit, herpes zoster vaccine, colon cancer screening, pelvic screening), functional status (accidents), and channeling. The 1-year relative risk (RR) for each NCO was estimated for all treatment comparisons using an inverse probability of treatment and censoring weighted estimator.
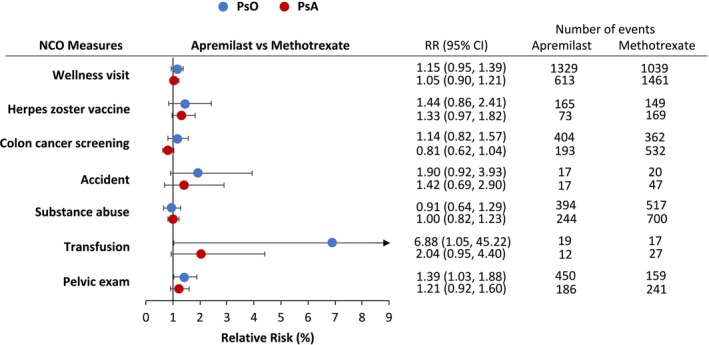
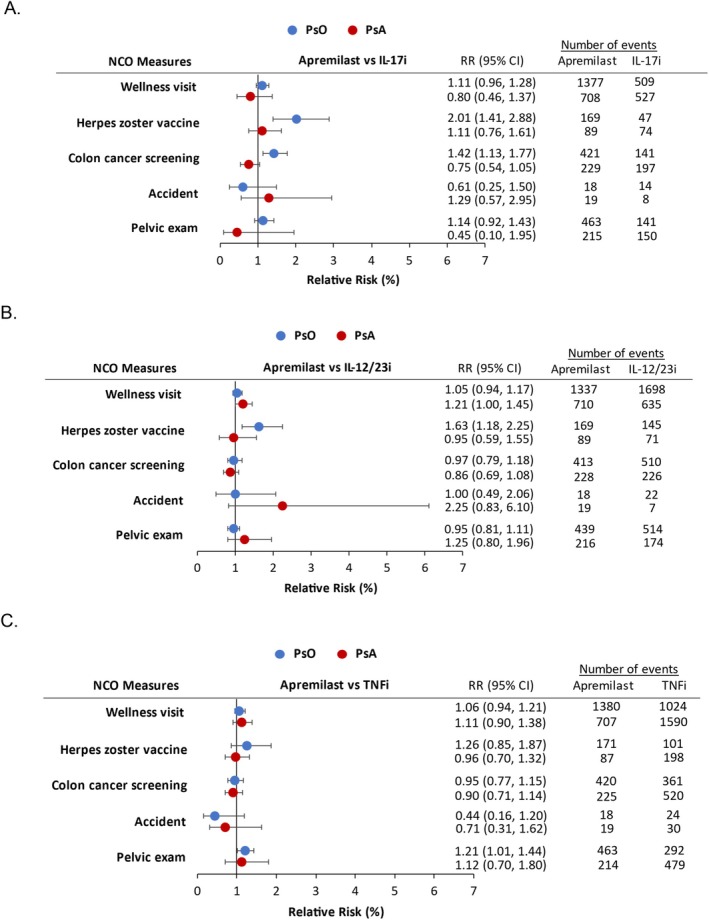
Results: In PsO, potential healthy user bias was detected in apremilast vs. IL-17i initiators, with a higher likelihood of herpes zoster vaccine and colon cancer screening (RR [95% CI]: 2.01 [1.41, 2.88] and 1.42 [1.13, 1.77], respectively). Wellness visits and pelvic exams were less likely among apremilast vs. topical initiators (0.84 [0.72, 0.98] and 0.83 [0.70, 0.98], respectively). The wellness visit RR was attenuated in individuals with ≥ 1 pre-index topical prescription (0.90 [0.78, 1.04]). In PsA, minimal residual confounding was observed between apremilast and other treatments.
Conclusions: Eligibility criteria (prior topicals) and weighting reduced residual confounding when comparing apremilast vs. other treatments for PsO and PsA. Integration of NCOs into comparative effectiveness/safety studies of PsO/PsA treatments may help identify unmeasured confounding.
期刊介绍:
The aim of Pharmacoepidemiology and Drug Safety is to provide an international forum for the communication and evaluation of data, methods and opinion in the discipline of pharmacoepidemiology. The Journal publishes peer-reviewed reports of original research, invited reviews and a variety of guest editorials and commentaries embracing scientific, medical, statistical, legal and economic aspects of pharmacoepidemiology and post-marketing surveillance of drug safety. Appropriate material in these categories may also be considered for publication as a Brief Report.
Particular areas of interest include:
design, analysis, results, and interpretation of studies looking at the benefit or safety of specific pharmaceuticals, biologics, or medical devices, including studies in pharmacovigilance, postmarketing surveillance, pharmacoeconomics, patient safety, molecular pharmacoepidemiology, or any other study within the broad field of pharmacoepidemiology;
comparative effectiveness research relating to pharmaceuticals, biologics, and medical devices. Comparative effectiveness research is the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, as these methods are truly used in the real world;
methodologic contributions of relevance to pharmacoepidemiology, whether original contributions, reviews of existing methods, or tutorials for how to apply the methods of pharmacoepidemiology;
assessments of harm versus benefit in drug therapy;
patterns of drug utilization;
relationships between pharmacoepidemiology and the formulation and interpretation of regulatory guidelines;
evaluations of risk management plans and programmes relating to pharmaceuticals, biologics and medical devices.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


