Alexa Pichet Binette, Ruben Smith, Gemma Salvadó, Pontus Tideman, Isabelle Glans, Danielle van Westen, Colin Groot, Rik Ossenkoppele, Erik Stomrud, Piero Parchi, Henrik Zetterberg, Kaj Blennow, Niklas Mattsson-Carlgren, Shorena Janelidze, Sebastian Palmqvist, Oskar Hansson
{"title":"阿尔茨海默病生物学和临床分期修订标准的评价。","authors":"Alexa Pichet Binette, Ruben Smith, Gemma Salvadó, Pontus Tideman, Isabelle Glans, Danielle van Westen, Colin Groot, Rik Ossenkoppele, Erik Stomrud, Piero Parchi, Henrik Zetterberg, Kaj Blennow, Niklas Mattsson-Carlgren, Shorena Janelidze, Sebastian Palmqvist, Oskar Hansson","doi":"10.1001/jamaneurol.2025.1100","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>While clinical disease stages remained largely unchanged in the 2024 update of the Alzheimer disease (AD) criteria, tau-positron emission tomography (PET) was introduced as a core biomarker and its spatial extent was incorporated into the revised biological stages of the disease. It is important to consider both the clinical and the biological stages and understand their discrepancies.</p><p><strong>Objective: </strong>To compare individuals who have discrepant biological and clinical stages with those who have congruent stages in terms of copathologies, comorbidities, and demographics.</p><p><strong>Design, setting, and participants: </strong>Participants were from the Swedish BioFINDER-2 (inclusion from 2017 through 2023) and the Alzheimer's Disease Neuroimaging Initiative (ADNI) (inclusion from 2015 through 2024). BioFINDER-2 included a prospective population-based (cognitively normal [CN] older adults) and memory clinic-based cohort (participants with subjective cognitive impairment [SCD], mild cognitive impairment [MCI], and dementia). ADNI included a volunteer-based sample. All participants who were amyloid-β positive and had undergone tau-PET were included. In BioFINDER-2, 838 participants of a total of 1979 were included, and of 927 with tau-PET in ADNI, 380 were included.</p><p><strong>Exposures: </strong>The clinical (CN to dementia) and biological (based on PET; initial [amyloid-β-positive only] to advanced [amyloid-β-positive, elevated, and widespread tau]) stages from the revised AD criteria.</p><p><strong>Main outcomes and measures: </strong>Cross-sectional measures of neurodegeneration (cortical thickness, TAR DNA-binding protein 43 [TDP-43] imaging signature, neurofilament light [NfL]), α-synuclein cerebrospinal fluid status, plasma glial fibrillary acidic protein, white matter lesions, infarcts, microbleeds, comorbidities, and demographics.</p><p><strong>Results: </strong>There were 838 BioFINDER-2 participants (mean age, 73.9 [SD, 7.3] years; 431 women [51%]; 407 men [49%]) and 380 ADNI participants (average age, 72.9 [SD, 7.0] years; 194 women [51%]; 186 mean [49%]) included. In BioFINDER-2, 37.7% of the sample had congruent biological and clinical stages (reference group), 51.3% had more advanced clinical impairment compared with their clinical stage (clinical > biological) and 11.0% had the opposite (biological > clinical). The main differences were between the reference group and the clinical > biological group: the latter participants were more often positive for α-synuclein pathology, had higher NfL levels, greater TDP-43-like atrophy, and higher burden of cerebral small vessel disease lesions (all false discovery rate P < .05). The only difference between the biological > clinical and the reference group was that the former had less neurodegeneration (thicker cortex; all false discovery rate P < .001). The main results were replicated in the independent ADNI cohort, where congruent 56.1% of participants had biological and clinical stages; 36.1% were in the category clinical > biological, and 7.9% in biological > clinical.</p><p><strong>Conclusions and relevance: </strong>Copathologies play an important role in symptom severity in individuals who harbor less tau-tangle pathology than expected for their clinical impairment. These results highlight the importance of measuring non-AD biomarkers in patients with AD with worse cognitive impairment than expected based on their biological stage, which could impact the clinical diagnosis and prognosis.</p>","PeriodicalId":14677,"journal":{"name":"JAMA neurology","volume":" ","pages":"666-675"},"PeriodicalIF":21.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12090069/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of the Revised Criteria for Biological and Clinical Staging of Alzheimer Disease.\",\"authors\":\"Alexa Pichet Binette, Ruben Smith, Gemma Salvadó, Pontus Tideman, Isabelle Glans, Danielle van Westen, Colin Groot, Rik Ossenkoppele, Erik Stomrud, Piero Parchi, Henrik Zetterberg, Kaj Blennow, Niklas Mattsson-Carlgren, Shorena Janelidze, Sebastian Palmqvist, Oskar Hansson\",\"doi\":\"10.1001/jamaneurol.2025.1100\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>While clinical disease stages remained largely unchanged in the 2024 update of the Alzheimer disease (AD) criteria, tau-positron emission tomography (PET) was introduced as a core biomarker and its spatial extent was incorporated into the revised biological stages of the disease. It is important to consider both the clinical and the biological stages and understand their discrepancies.</p><p><strong>Objective: </strong>To compare individuals who have discrepant biological and clinical stages with those who have congruent stages in terms of copathologies, comorbidities, and demographics.</p><p><strong>Design, setting, and participants: </strong>Participants were from the Swedish BioFINDER-2 (inclusion from 2017 through 2023) and the Alzheimer's Disease Neuroimaging Initiative (ADNI) (inclusion from 2015 through 2024). BioFINDER-2 included a prospective population-based (cognitively normal [CN] older adults) and memory clinic-based cohort (participants with subjective cognitive impairment [SCD], mild cognitive impairment [MCI], and dementia). ADNI included a volunteer-based sample. All participants who were amyloid-β positive and had undergone tau-PET were included. In BioFINDER-2, 838 participants of a total of 1979 were included, and of 927 with tau-PET in ADNI, 380 were included.</p><p><strong>Exposures: </strong>The clinical (CN to dementia) and biological (based on PET; initial [amyloid-β-positive only] to advanced [amyloid-β-positive, elevated, and widespread tau]) stages from the revised AD criteria.</p><p><strong>Main outcomes and measures: </strong>Cross-sectional measures of neurodegeneration (cortical thickness, TAR DNA-binding protein 43 [TDP-43] imaging signature, neurofilament light [NfL]), α-synuclein cerebrospinal fluid status, plasma glial fibrillary acidic protein, white matter lesions, infarcts, microbleeds, comorbidities, and demographics.</p><p><strong>Results: </strong>There were 838 BioFINDER-2 participants (mean age, 73.9 [SD, 7.3] years; 431 women [51%]; 407 men [49%]) and 380 ADNI participants (average age, 72.9 [SD, 7.0] years; 194 women [51%]; 186 mean [49%]) included. In BioFINDER-2, 37.7% of the sample had congruent biological and clinical stages (reference group), 51.3% had more advanced clinical impairment compared with their clinical stage (clinical > biological) and 11.0% had the opposite (biological > clinical). The main differences were between the reference group and the clinical > biological group: the latter participants were more often positive for α-synuclein pathology, had higher NfL levels, greater TDP-43-like atrophy, and higher burden of cerebral small vessel disease lesions (all false discovery rate P < .05). The only difference between the biological > clinical and the reference group was that the former had less neurodegeneration (thicker cortex; all false discovery rate P < .001). The main results were replicated in the independent ADNI cohort, where congruent 56.1% of participants had biological and clinical stages; 36.1% were in the category clinical > biological, and 7.9% in biological > clinical.</p><p><strong>Conclusions and relevance: </strong>Copathologies play an important role in symptom severity in individuals who harbor less tau-tangle pathology than expected for their clinical impairment. These results highlight the importance of measuring non-AD biomarkers in patients with AD with worse cognitive impairment than expected based on their biological stage, which could impact the clinical diagnosis and prognosis.</p>\",\"PeriodicalId\":14677,\"journal\":{\"name\":\"JAMA neurology\",\"volume\":\" \",\"pages\":\"666-675\"},\"PeriodicalIF\":21.3000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12090069/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA neurology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1001/jamaneurol.2025.1100\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamaneurol.2025.1100","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Evaluation of the Revised Criteria for Biological and Clinical Staging of Alzheimer Disease.
Importance: While clinical disease stages remained largely unchanged in the 2024 update of the Alzheimer disease (AD) criteria, tau-positron emission tomography (PET) was introduced as a core biomarker and its spatial extent was incorporated into the revised biological stages of the disease. It is important to consider both the clinical and the biological stages and understand their discrepancies.
Objective: To compare individuals who have discrepant biological and clinical stages with those who have congruent stages in terms of copathologies, comorbidities, and demographics.
Design, setting, and participants: Participants were from the Swedish BioFINDER-2 (inclusion from 2017 through 2023) and the Alzheimer's Disease Neuroimaging Initiative (ADNI) (inclusion from 2015 through 2024). BioFINDER-2 included a prospective population-based (cognitively normal [CN] older adults) and memory clinic-based cohort (participants with subjective cognitive impairment [SCD], mild cognitive impairment [MCI], and dementia). ADNI included a volunteer-based sample. All participants who were amyloid-β positive and had undergone tau-PET were included. In BioFINDER-2, 838 participants of a total of 1979 were included, and of 927 with tau-PET in ADNI, 380 were included.
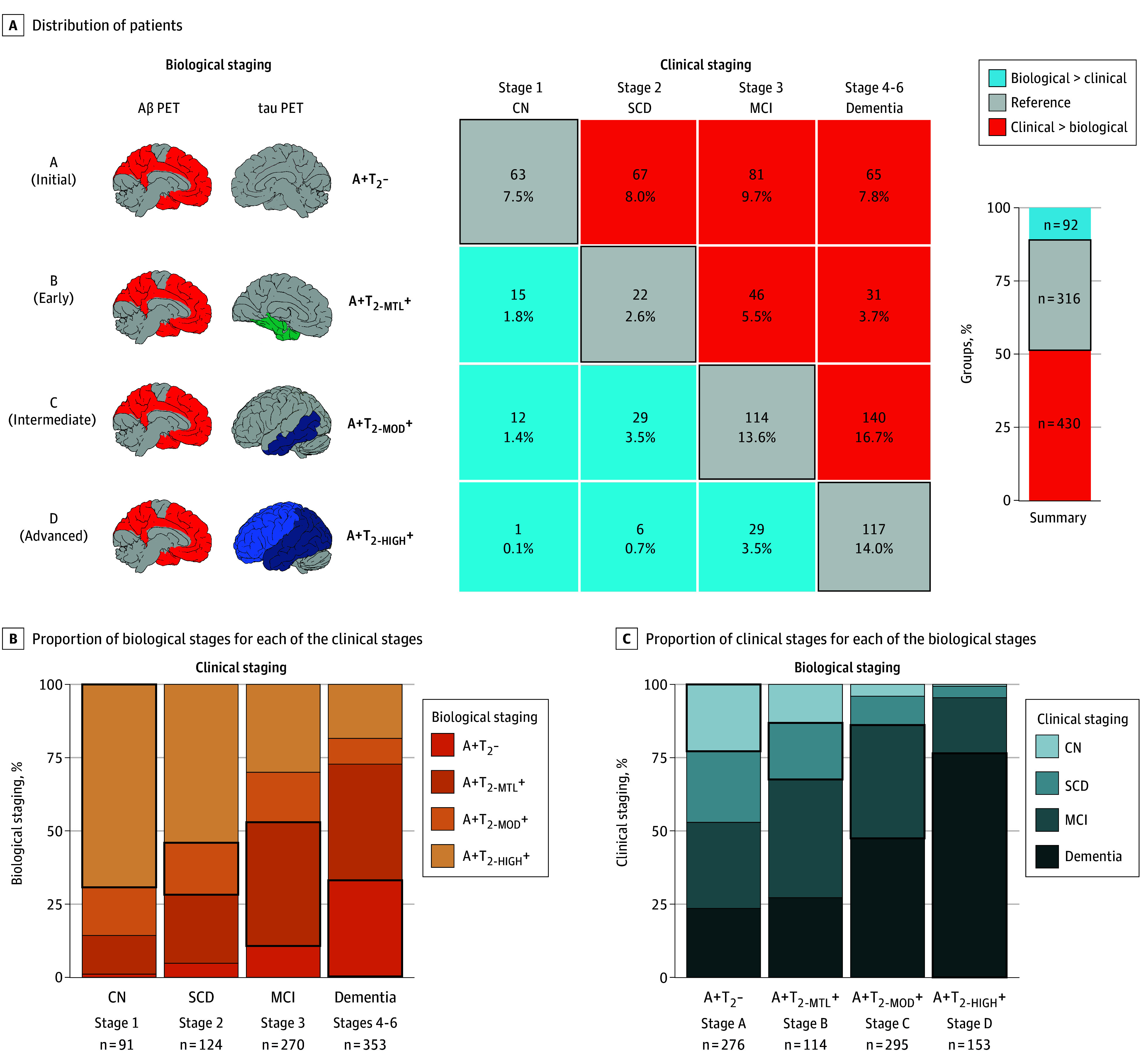
Exposures: The clinical (CN to dementia) and biological (based on PET; initial [amyloid-β-positive only] to advanced [amyloid-β-positive, elevated, and widespread tau]) stages from the revised AD criteria.
Main outcomes and measures: Cross-sectional measures of neurodegeneration (cortical thickness, TAR DNA-binding protein 43 [TDP-43] imaging signature, neurofilament light [NfL]), α-synuclein cerebrospinal fluid status, plasma glial fibrillary acidic protein, white matter lesions, infarcts, microbleeds, comorbidities, and demographics.
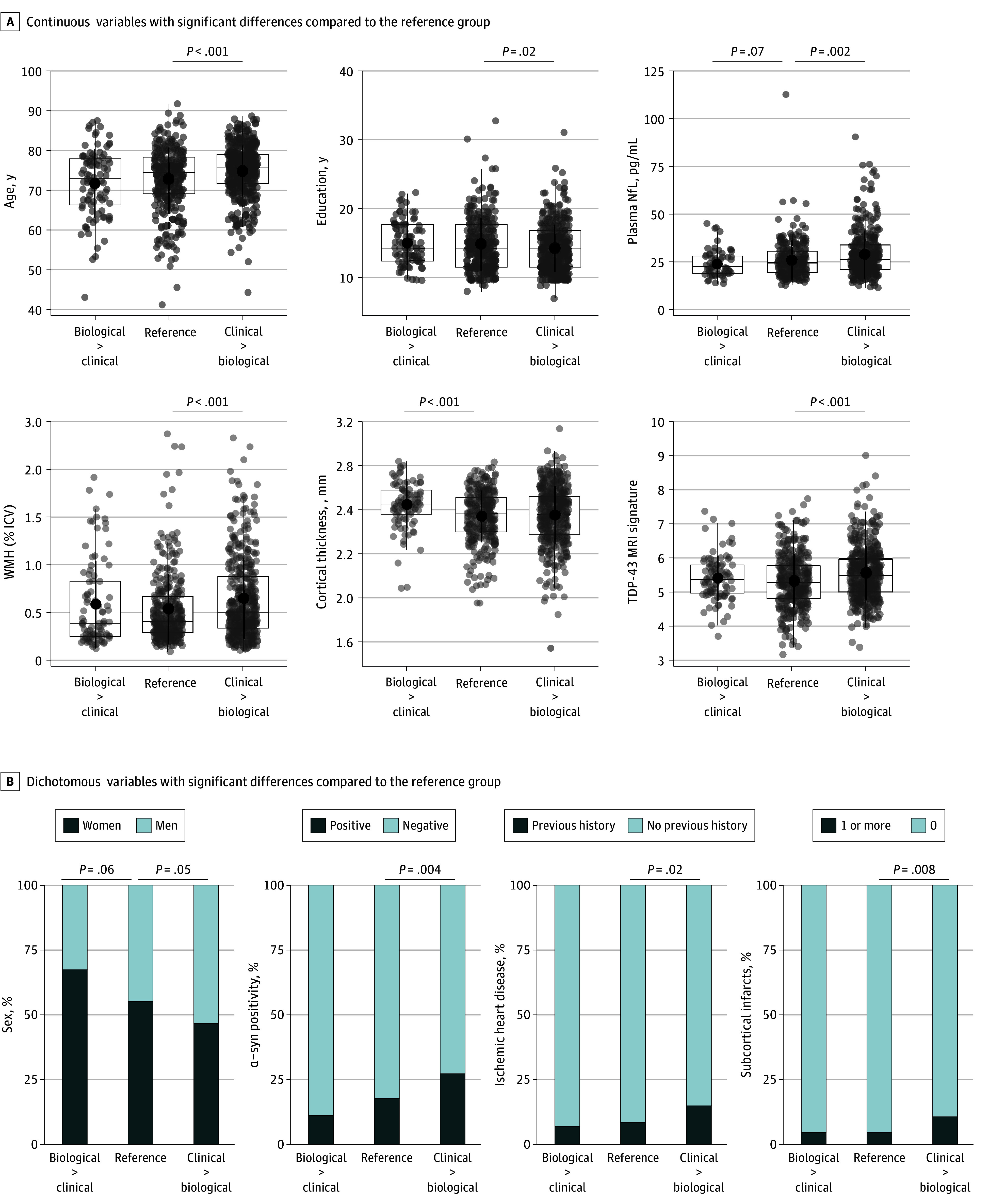
Results: There were 838 BioFINDER-2 participants (mean age, 73.9 [SD, 7.3] years; 431 women [51%]; 407 men [49%]) and 380 ADNI participants (average age, 72.9 [SD, 7.0] years; 194 women [51%]; 186 mean [49%]) included. In BioFINDER-2, 37.7% of the sample had congruent biological and clinical stages (reference group), 51.3% had more advanced clinical impairment compared with their clinical stage (clinical > biological) and 11.0% had the opposite (biological > clinical). The main differences were between the reference group and the clinical > biological group: the latter participants were more often positive for α-synuclein pathology, had higher NfL levels, greater TDP-43-like atrophy, and higher burden of cerebral small vessel disease lesions (all false discovery rate P < .05). The only difference between the biological > clinical and the reference group was that the former had less neurodegeneration (thicker cortex; all false discovery rate P < .001). The main results were replicated in the independent ADNI cohort, where congruent 56.1% of participants had biological and clinical stages; 36.1% were in the category clinical > biological, and 7.9% in biological > clinical.
Conclusions and relevance: Copathologies play an important role in symptom severity in individuals who harbor less tau-tangle pathology than expected for their clinical impairment. These results highlight the importance of measuring non-AD biomarkers in patients with AD with worse cognitive impairment than expected based on their biological stage, which could impact the clinical diagnosis and prognosis.
期刊介绍:
JAMA Neurology is an international peer-reviewed journal for physicians caring for people with neurologic disorders and those interested in the structure and function of the normal and diseased nervous system. The Archives of Neurology & Psychiatry began publication in 1919 and, in 1959, became 2 separate journals: Archives of Neurology and Archives of General Psychiatry. In 2013, their names changed to JAMA Neurology and JAMA Psychiatry, respectively. JAMA Neurology is a member of the JAMA Network, a consortium of peer-reviewed, general medical and specialty publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


