Tobias Giertzsch, Michael Jerosch-Herold, Philipp Schneider, Inga Voges, Dominik Daniel Gabbert, Philip Wegner, Götz Müller, Tilo Kölbel, Ida Hüners, Jörg Siegmar Sachweh, Michael Hübler, Jochen Herrmann, Sophie Alt, Anne Schöber, Inka Ristow, Gerhard Adam, Gunnar K Lund, Carsten Rickers
{"title":"儿童和年轻人主动脉缩窄的无创组织特征——一项基于mri的前瞻性研究。","authors":"Tobias Giertzsch, Michael Jerosch-Herold, Philipp Schneider, Inga Voges, Dominik Daniel Gabbert, Philip Wegner, Götz Müller, Tilo Kölbel, Ida Hüners, Jörg Siegmar Sachweh, Michael Hübler, Jochen Herrmann, Sophie Alt, Anne Schöber, Inka Ristow, Gerhard Adam, Gunnar K Lund, Carsten Rickers","doi":"10.21037/cdt-24-497","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Aortic coarctation (CoA) necessitates long-term monitoring to identify late complications, including re-stenosis, aneurysms, arrhythmias and heart failure. Nonetheless, there remain gaps in understanding the effects of adverse left-ventricular (LV) remodeling at the myocardial tissue level, which may contribute to incipient heart failure. The aim of this study is to evaluate myocardial tissue characteristics in patients with CoA using advanced cardiac magnetic resonance (CMR) imaging techniques to identify markers of adverse tissue remodeling and their association with disease severity, bicuspid aortic valve (BAV), and clinical management strategies such as blood pressure (BP) medication.</p><p><strong>Methods: </strong>CMR imaging at 3 Tesla was used to determine the myocardial extracellular volume fraction (ECV), native T1, and intracellular water lifetime (τ<sub>ic</sub>) by pre- and post-gadolinium contrast T1 mapping in 46 patients (21 male; mean age 20 years) with CoA and 14 age-matched controls. LV volumes, mass, and ejection fraction were obtained from cine CMR. CoA was classified as low grade [\"LG\" = the maximum flow velocity (Vmax) ≤3 m/s and no re-stenosis, nor arterial hypertension or medication], severe CoA (\"sCoA\" = Vmax >3 m/s or one of LG's other variables applies), and \"CoA with BAV\".</p><p><strong>Results: </strong>ECV was significantly higher in sCoA group (0.31±0.04) compared to LG group (0.26±0.02, P=0.002) and healthy controls (0.26±0.02, P=0.001). ECV with BAV (0.31±0.05) was higher than in LG group (P=0.03) and healthy controls (P=0.03). Native T1 values were significantly elevated in sCoA group (T1 =1,391±162 ms) compared to LG group (T1 =1,213±47 ms, P=0.002) and in CoA with BAV (T1 =1,390±127 ms) versus LG group (P=0.002). τ<sub>ic</sub> was lower in LG group (0.24±0.03 s), indicative of a smaller cardiomyocyte diameter, compared to sCoA (0.28±0.04 s; P=0.01) and LG CoA with concomitant BAV (0.31±0.05 s; P=0.04). The LV end-systolic volume (ESV) was significantly higher in group with BAV than in LG CoA (P<0.001) and sCoA (P=0.001) groups. Patients who took BP medication had significantly lower values in native T1 (P=0.02) and τ<sub>ic</sub> (P=0.03).</p><p><strong>Conclusions: </strong>sCoA is associated with an elevated myocardial ECV and native T1 compared to LG CoAs and healthy controls, reflecting adverse tissue remodeling. Patients with LG CoA and concomitant BAV showed significantly greater diffuse myocardial fibrosis than those with isolated LG CoA. CoA patients, especially those with sCoA and those with concomitant BAV, could be at increased long-term risk for complications related to diffuse myocardial fibrosis, such as diastolic dysfunction and arrhythmias. Patients taking antihypertensive medication may benefit from reduced cardiomyocyte hypertrophy and less interstitial fibrosis.</p>","PeriodicalId":9592,"journal":{"name":"Cardiovascular diagnosis and therapy","volume":"15 2","pages":"375-387"},"PeriodicalIF":2.1000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082215/pdf/","citationCount":"0","resultStr":"{\"title\":\"Non-invasive tissue characterization in children and young adults with aortic coarctation-an MRI-based prospective study.\",\"authors\":\"Tobias Giertzsch, Michael Jerosch-Herold, Philipp Schneider, Inga Voges, Dominik Daniel Gabbert, Philip Wegner, Götz Müller, Tilo Kölbel, Ida Hüners, Jörg Siegmar Sachweh, Michael Hübler, Jochen Herrmann, Sophie Alt, Anne Schöber, Inka Ristow, Gerhard Adam, Gunnar K Lund, Carsten Rickers\",\"doi\":\"10.21037/cdt-24-497\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Aortic coarctation (CoA) necessitates long-term monitoring to identify late complications, including re-stenosis, aneurysms, arrhythmias and heart failure. Nonetheless, there remain gaps in understanding the effects of adverse left-ventricular (LV) remodeling at the myocardial tissue level, which may contribute to incipient heart failure. The aim of this study is to evaluate myocardial tissue characteristics in patients with CoA using advanced cardiac magnetic resonance (CMR) imaging techniques to identify markers of adverse tissue remodeling and their association with disease severity, bicuspid aortic valve (BAV), and clinical management strategies such as blood pressure (BP) medication.</p><p><strong>Methods: </strong>CMR imaging at 3 Tesla was used to determine the myocardial extracellular volume fraction (ECV), native T1, and intracellular water lifetime (τ<sub>ic</sub>) by pre- and post-gadolinium contrast T1 mapping in 46 patients (21 male; mean age 20 years) with CoA and 14 age-matched controls. LV volumes, mass, and ejection fraction were obtained from cine CMR. CoA was classified as low grade [\\\"LG\\\" = the maximum flow velocity (Vmax) ≤3 m/s and no re-stenosis, nor arterial hypertension or medication], severe CoA (\\\"sCoA\\\" = Vmax >3 m/s or one of LG's other variables applies), and \\\"CoA with BAV\\\".</p><p><strong>Results: </strong>ECV was significantly higher in sCoA group (0.31±0.04) compared to LG group (0.26±0.02, P=0.002) and healthy controls (0.26±0.02, P=0.001). ECV with BAV (0.31±0.05) was higher than in LG group (P=0.03) and healthy controls (P=0.03). Native T1 values were significantly elevated in sCoA group (T1 =1,391±162 ms) compared to LG group (T1 =1,213±47 ms, P=0.002) and in CoA with BAV (T1 =1,390±127 ms) versus LG group (P=0.002). τ<sub>ic</sub> was lower in LG group (0.24±0.03 s), indicative of a smaller cardiomyocyte diameter, compared to sCoA (0.28±0.04 s; P=0.01) and LG CoA with concomitant BAV (0.31±0.05 s; P=0.04). The LV end-systolic volume (ESV) was significantly higher in group with BAV than in LG CoA (P<0.001) and sCoA (P=0.001) groups. Patients who took BP medication had significantly lower values in native T1 (P=0.02) and τ<sub>ic</sub> (P=0.03).</p><p><strong>Conclusions: </strong>sCoA is associated with an elevated myocardial ECV and native T1 compared to LG CoAs and healthy controls, reflecting adverse tissue remodeling. Patients with LG CoA and concomitant BAV showed significantly greater diffuse myocardial fibrosis than those with isolated LG CoA. CoA patients, especially those with sCoA and those with concomitant BAV, could be at increased long-term risk for complications related to diffuse myocardial fibrosis, such as diastolic dysfunction and arrhythmias. Patients taking antihypertensive medication may benefit from reduced cardiomyocyte hypertrophy and less interstitial fibrosis.</p>\",\"PeriodicalId\":9592,\"journal\":{\"name\":\"Cardiovascular diagnosis and therapy\",\"volume\":\"15 2\",\"pages\":\"375-387\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082215/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiovascular diagnosis and therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/cdt-24-497\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular diagnosis and therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/cdt-24-497","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Non-invasive tissue characterization in children and young adults with aortic coarctation-an MRI-based prospective study.
Background: Aortic coarctation (CoA) necessitates long-term monitoring to identify late complications, including re-stenosis, aneurysms, arrhythmias and heart failure. Nonetheless, there remain gaps in understanding the effects of adverse left-ventricular (LV) remodeling at the myocardial tissue level, which may contribute to incipient heart failure. The aim of this study is to evaluate myocardial tissue characteristics in patients with CoA using advanced cardiac magnetic resonance (CMR) imaging techniques to identify markers of adverse tissue remodeling and their association with disease severity, bicuspid aortic valve (BAV), and clinical management strategies such as blood pressure (BP) medication.
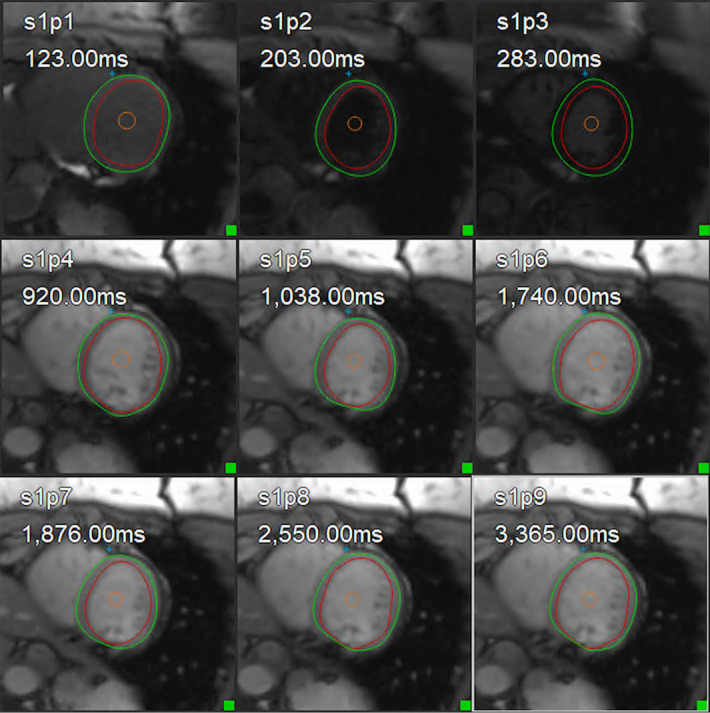
Methods: CMR imaging at 3 Tesla was used to determine the myocardial extracellular volume fraction (ECV), native T1, and intracellular water lifetime (τic) by pre- and post-gadolinium contrast T1 mapping in 46 patients (21 male; mean age 20 years) with CoA and 14 age-matched controls. LV volumes, mass, and ejection fraction were obtained from cine CMR. CoA was classified as low grade ["LG" = the maximum flow velocity (Vmax) ≤3 m/s and no re-stenosis, nor arterial hypertension or medication], severe CoA ("sCoA" = Vmax >3 m/s or one of LG's other variables applies), and "CoA with BAV".
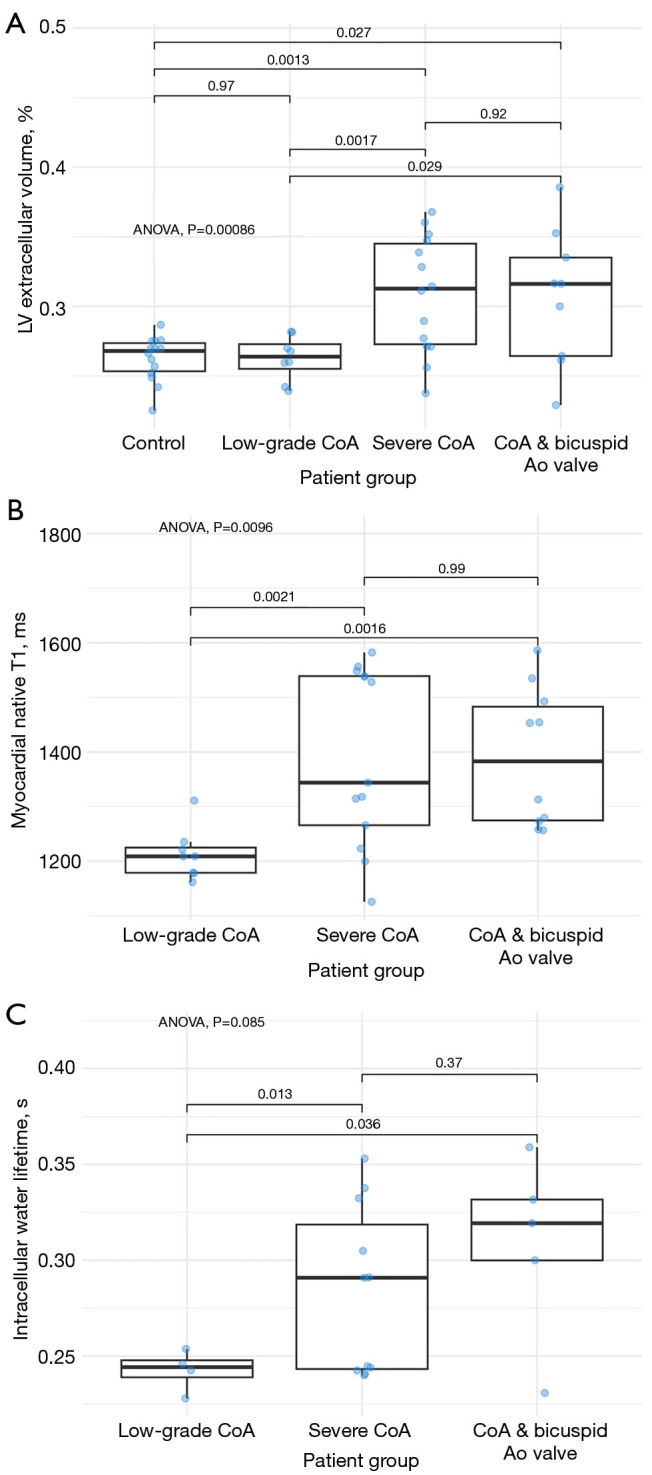
Results: ECV was significantly higher in sCoA group (0.31±0.04) compared to LG group (0.26±0.02, P=0.002) and healthy controls (0.26±0.02, P=0.001). ECV with BAV (0.31±0.05) was higher than in LG group (P=0.03) and healthy controls (P=0.03). Native T1 values were significantly elevated in sCoA group (T1 =1,391±162 ms) compared to LG group (T1 =1,213±47 ms, P=0.002) and in CoA with BAV (T1 =1,390±127 ms) versus LG group (P=0.002). τic was lower in LG group (0.24±0.03 s), indicative of a smaller cardiomyocyte diameter, compared to sCoA (0.28±0.04 s; P=0.01) and LG CoA with concomitant BAV (0.31±0.05 s; P=0.04). The LV end-systolic volume (ESV) was significantly higher in group with BAV than in LG CoA (P<0.001) and sCoA (P=0.001) groups. Patients who took BP medication had significantly lower values in native T1 (P=0.02) and τic (P=0.03).
Conclusions: sCoA is associated with an elevated myocardial ECV and native T1 compared to LG CoAs and healthy controls, reflecting adverse tissue remodeling. Patients with LG CoA and concomitant BAV showed significantly greater diffuse myocardial fibrosis than those with isolated LG CoA. CoA patients, especially those with sCoA and those with concomitant BAV, could be at increased long-term risk for complications related to diffuse myocardial fibrosis, such as diastolic dysfunction and arrhythmias. Patients taking antihypertensive medication may benefit from reduced cardiomyocyte hypertrophy and less interstitial fibrosis.
期刊介绍:
The journal ''Cardiovascular Diagnosis and Therapy'' (Print ISSN: 2223-3652; Online ISSN: 2223-3660) accepts basic and clinical science submissions related to Cardiovascular Medicine and Surgery. The mission of the journal is the rapid exchange of scientific information between clinicians and scientists worldwide. To reach this goal, the journal will focus on novel media, using a web-based, digital format in addition to traditional print-version. This includes on-line submission, review, publication, and distribution. The digital format will also allow submission of extensive supporting visual material, both images and video. The website www.thecdt.org will serve as the central hub and also allow posting of comments and on-line discussion. The web-site of the journal will be linked to a number of international web-sites (e.g. www.dxy.cn), which will significantly expand the distribution of its contents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


