J E Griggs, S Clarke, R Greenhalgh, A N Watts, J Barrett, S Houghton Budd, M Dias, K Hunter, R M Lyon, E Ter Avest
{"title":"院前有创动脉血压监测对外伤性脑损伤和自发性颅内出血血流动力学治疗的诊断准确性。","authors":"J E Griggs, S Clarke, R Greenhalgh, A N Watts, J Barrett, S Houghton Budd, M Dias, K Hunter, R M Lyon, E Ter Avest","doi":"10.1186/s13049-025-01393-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neuroprotective measures to prevent secondary brain injury are a critical aspect of pre-hospital management in patients with acute traumatic brain injury (TBI) and spontaneous intracranial haemorrhage (sICH). Haemodynamic optimisation guided by non-invasive blood pressure (NIBP) measurements is an important neuroprotective measure, as cerebral autoregulation is often absent or impaired. The accuracy and clinical relevance of invasive arterial blood pressure (IBP) monitoring to optimise haemodynamic management has not been established in patients with a brain insult.</p><p><strong>Methods: </strong>A retrospective clinical diagnostic accuracy study to establish the accuracy and clinical relevance of IBP-guided haemodynamic optimisation in patients with TBI or sICH. The occurrence- and clinical relevance of IBP-NIBP discrepancies in patients attended by a UK Helicopter Emergency Medical Service (HEMS) between 6 January 2022 and 6 January 2024 was evaluated. Bland-Altman plots with adjustment for repeated measures were constructed to analyse disagreement in relation to absolute blood pressure values. Multivariate analysis was performed using generalised linear mixed effects regression (GLMER) models with random effects to identify predictors of disagreement. Error Grid Analysis (EGA) classified the clinical relevance of discrepancies. The primary outcome was pairwise agreement between IBP and NIBP, defined as less than 10% difference in mean arterial pressure (MAP).</p><p><strong>Results: </strong>For 209 patients (159 TBI and 50 sICH) 1020 concurrent IBP and NIBP measurements were available. The average [95% CI] difference in MAP was -1.4 mmHg (-3.09 to 0.27) and 2.6mmHg in TBI. Only 459 (54.7%) MAP data met criteria for pairwise agreement. Multivariate regression analysis revealed a strong association between MAP disagreement and ground emergency medical service conveyance (aOR 2.01, 95% CI 0.98-4.10). Bland-Altman analysis demonstrated proportional bias, with NIBP underestimation of MAP at higher blood pressures and overestimation at lower blood pressures. EGA revealed that in 6.1% (95% CI: 4.5-7.7) of TBI and 12.5% (95% CI: 7.8-17.2) of patients with sICH pairwise disagreement was associated with a moderate to dangerous risk of over- or undertreatment.</p><p><strong>Conclusion: </strong>NIBP guided pre-hospital haemodynamic management of patients with TBI or sICH is hampered by clinically relevant measurement inaccuracies in a significant proportion of patients. Pre-hospital IBP has the potential to improve early haemodynamic optimisation, especially when hypo- or hypertension is present, enabling tailored neuroprotection in the hyperacute phase.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"89"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082994/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnostic accuracy of pre-hospital invasive arterial blood pressure monitoring for haemodynamic management in traumatic brain injury and spontaneous intracranial haemorrhage.\",\"authors\":\"J E Griggs, S Clarke, R Greenhalgh, A N Watts, J Barrett, S Houghton Budd, M Dias, K Hunter, R M Lyon, E Ter Avest\",\"doi\":\"10.1186/s13049-025-01393-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Neuroprotective measures to prevent secondary brain injury are a critical aspect of pre-hospital management in patients with acute traumatic brain injury (TBI) and spontaneous intracranial haemorrhage (sICH). Haemodynamic optimisation guided by non-invasive blood pressure (NIBP) measurements is an important neuroprotective measure, as cerebral autoregulation is often absent or impaired. The accuracy and clinical relevance of invasive arterial blood pressure (IBP) monitoring to optimise haemodynamic management has not been established in patients with a brain insult.</p><p><strong>Methods: </strong>A retrospective clinical diagnostic accuracy study to establish the accuracy and clinical relevance of IBP-guided haemodynamic optimisation in patients with TBI or sICH. The occurrence- and clinical relevance of IBP-NIBP discrepancies in patients attended by a UK Helicopter Emergency Medical Service (HEMS) between 6 January 2022 and 6 January 2024 was evaluated. Bland-Altman plots with adjustment for repeated measures were constructed to analyse disagreement in relation to absolute blood pressure values. Multivariate analysis was performed using generalised linear mixed effects regression (GLMER) models with random effects to identify predictors of disagreement. Error Grid Analysis (EGA) classified the clinical relevance of discrepancies. The primary outcome was pairwise agreement between IBP and NIBP, defined as less than 10% difference in mean arterial pressure (MAP).</p><p><strong>Results: </strong>For 209 patients (159 TBI and 50 sICH) 1020 concurrent IBP and NIBP measurements were available. The average [95% CI] difference in MAP was -1.4 mmHg (-3.09 to 0.27) and 2.6mmHg in TBI. Only 459 (54.7%) MAP data met criteria for pairwise agreement. Multivariate regression analysis revealed a strong association between MAP disagreement and ground emergency medical service conveyance (aOR 2.01, 95% CI 0.98-4.10). Bland-Altman analysis demonstrated proportional bias, with NIBP underestimation of MAP at higher blood pressures and overestimation at lower blood pressures. EGA revealed that in 6.1% (95% CI: 4.5-7.7) of TBI and 12.5% (95% CI: 7.8-17.2) of patients with sICH pairwise disagreement was associated with a moderate to dangerous risk of over- or undertreatment.</p><p><strong>Conclusion: </strong>NIBP guided pre-hospital haemodynamic management of patients with TBI or sICH is hampered by clinically relevant measurement inaccuracies in a significant proportion of patients. Pre-hospital IBP has the potential to improve early haemodynamic optimisation, especially when hypo- or hypertension is present, enabling tailored neuroprotection in the hyperacute phase.</p>\",\"PeriodicalId\":49292,\"journal\":{\"name\":\"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine\",\"volume\":\"33 1\",\"pages\":\"89\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-05-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082994/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13049-025-01393-4\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01393-4","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Diagnostic accuracy of pre-hospital invasive arterial blood pressure monitoring for haemodynamic management in traumatic brain injury and spontaneous intracranial haemorrhage.
Background: Neuroprotective measures to prevent secondary brain injury are a critical aspect of pre-hospital management in patients with acute traumatic brain injury (TBI) and spontaneous intracranial haemorrhage (sICH). Haemodynamic optimisation guided by non-invasive blood pressure (NIBP) measurements is an important neuroprotective measure, as cerebral autoregulation is often absent or impaired. The accuracy and clinical relevance of invasive arterial blood pressure (IBP) monitoring to optimise haemodynamic management has not been established in patients with a brain insult.
Methods: A retrospective clinical diagnostic accuracy study to establish the accuracy and clinical relevance of IBP-guided haemodynamic optimisation in patients with TBI or sICH. The occurrence- and clinical relevance of IBP-NIBP discrepancies in patients attended by a UK Helicopter Emergency Medical Service (HEMS) between 6 January 2022 and 6 January 2024 was evaluated. Bland-Altman plots with adjustment for repeated measures were constructed to analyse disagreement in relation to absolute blood pressure values. Multivariate analysis was performed using generalised linear mixed effects regression (GLMER) models with random effects to identify predictors of disagreement. Error Grid Analysis (EGA) classified the clinical relevance of discrepancies. The primary outcome was pairwise agreement between IBP and NIBP, defined as less than 10% difference in mean arterial pressure (MAP).
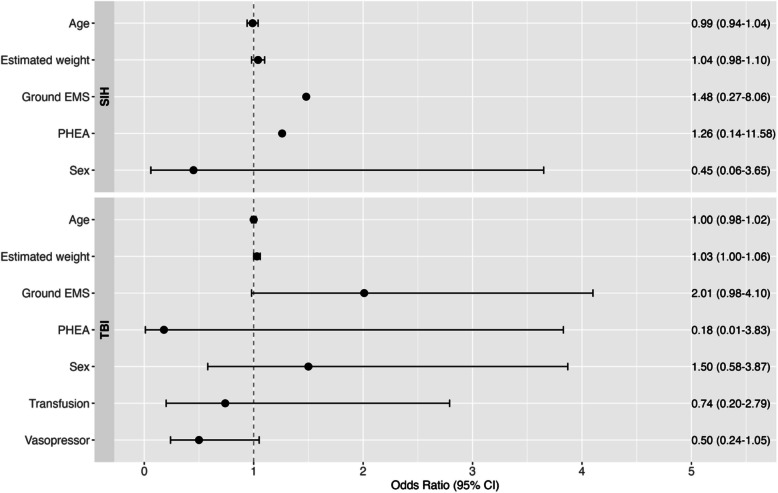
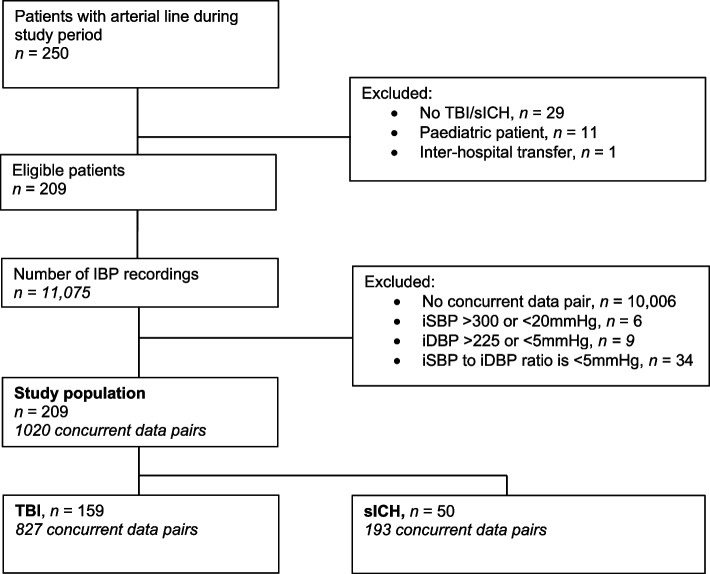
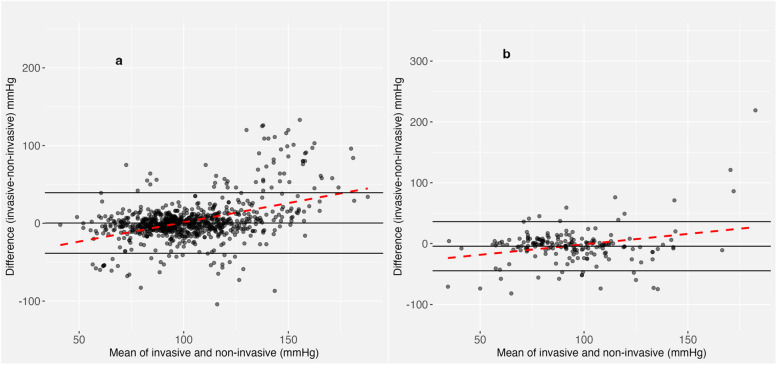
Results: For 209 patients (159 TBI and 50 sICH) 1020 concurrent IBP and NIBP measurements were available. The average [95% CI] difference in MAP was -1.4 mmHg (-3.09 to 0.27) and 2.6mmHg in TBI. Only 459 (54.7%) MAP data met criteria for pairwise agreement. Multivariate regression analysis revealed a strong association between MAP disagreement and ground emergency medical service conveyance (aOR 2.01, 95% CI 0.98-4.10). Bland-Altman analysis demonstrated proportional bias, with NIBP underestimation of MAP at higher blood pressures and overestimation at lower blood pressures. EGA revealed that in 6.1% (95% CI: 4.5-7.7) of TBI and 12.5% (95% CI: 7.8-17.2) of patients with sICH pairwise disagreement was associated with a moderate to dangerous risk of over- or undertreatment.
Conclusion: NIBP guided pre-hospital haemodynamic management of patients with TBI or sICH is hampered by clinically relevant measurement inaccuracies in a significant proportion of patients. Pre-hospital IBP has the potential to improve early haemodynamic optimisation, especially when hypo- or hypertension is present, enabling tailored neuroprotection in the hyperacute phase.
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


