Olga Zamulko, Vidhya Karivedu, Muhammad Kashif Riaz, Ilaina Monroe, Audrey Romano, Rachel Mulanda, Nicky Kurtzweil, Allie Forsythe, Casey L Allen, Nusrat Harun, Jianmin Pan, Shesh Rai, Dalia El-Gamal, Trisha M Wise-Draper
{"title":"评估尼拉帕尼和多斯塔利单抗(TSR-042)治疗复发/转移性头颈部鳞状细胞癌(HNSCC)患者疗效的II期研究。","authors":"Olga Zamulko, Vidhya Karivedu, Muhammad Kashif Riaz, Ilaina Monroe, Audrey Romano, Rachel Mulanda, Nicky Kurtzweil, Allie Forsythe, Casey L Allen, Nusrat Harun, Jianmin Pan, Shesh Rai, Dalia El-Gamal, Trisha M Wise-Draper","doi":"10.1158/2767-9764.CRC-25-0192","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC) portends a poor prognosis. DNA pathway repair mutations in HNSCC are associated with higher tumor mutational burden rates and immune checkpoint inhibitor response. PARP inhibitors (PARPi) induce ssDNA breaks and are efficacious in cancers with DNA repair defects. Thus, we designed a single-arm, open-label, phase II clinical trial to evaluate the combination of niraparib and dostarlimab in patients with R/M HNSCC.</p><p><strong>Patients and methods: </strong>Patients with R/M HNSCC were treated with niraparib and dostarlimab until disease progression or unacceptable toxicity. The primary endpoint was the overall response rate and clinical benefit assessed by RECIST version 1.1. Using Simon's two-step minimax design, 14 patients were planned to enroll in the first stage with a goal of overall clinical benefit of 50%.</p><p><strong>Results: </strong>Ten patients were enrolled. The majority were White males with a median age of 62.5. One patient had a PD-L1 combined positive score >20, a high tumor mutational burden, a BRCA1 rearrangement, and an ATRX splice site mutation. Nine patients previously failed anti-PD-1/PD-L1 therapy. The best overall response rate was 10%, with a 20% clinical benefit (1 partial response, 1 stable disease). The trial was terminated early for futility as the goal clinical benefit could not be reached. At a median follow-up of 10.13 months, the median progression-free survival was 3.8 months, and the median overall survival was 10.1 months. The most common grade 3 or higher treatment-related adverse events were thrombocytopenia and hypertension.</p><p><strong>Conclusions: </strong>The combination of niraparib and dostarlimab did not achieve the primary endpoint of clinical benefit, but activity may be improved with biomarker-driven treatment and selected patients.</p><p><strong>Significance: </strong>Patients with R/M HNSCC that progress on PD-1 inhibitors have poor prognoses. PARPis cause ssDNA breaks that accumulate in cells with mutations in DNA damage repair pathways, leading to synthetic lethality. However, PARPi also inhibits glycogen synthase kinase-3β activity, leading to upregulated PD-L1, which is abrogated by PD-1 inhibitors. In this study, we combine niraparib (PARPi) with dostarlimab (anti-PD-L1) to evaluate clinical benefit in patients with R/M HNSCC.</p>","PeriodicalId":72516,"journal":{"name":"Cancer research communications","volume":" ","pages":"939-944"},"PeriodicalIF":3.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12146980/pdf/","citationCount":"0","resultStr":"{\"title\":\"Phase II Study Evaluating the Efficacy of Niraparib and Dostarlimab (TSR-042) in Patients with Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma.\",\"authors\":\"Olga Zamulko, Vidhya Karivedu, Muhammad Kashif Riaz, Ilaina Monroe, Audrey Romano, Rachel Mulanda, Nicky Kurtzweil, Allie Forsythe, Casey L Allen, Nusrat Harun, Jianmin Pan, Shesh Rai, Dalia El-Gamal, Trisha M Wise-Draper\",\"doi\":\"10.1158/2767-9764.CRC-25-0192\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC) portends a poor prognosis. DNA pathway repair mutations in HNSCC are associated with higher tumor mutational burden rates and immune checkpoint inhibitor response. PARP inhibitors (PARPi) induce ssDNA breaks and are efficacious in cancers with DNA repair defects. Thus, we designed a single-arm, open-label, phase II clinical trial to evaluate the combination of niraparib and dostarlimab in patients with R/M HNSCC.</p><p><strong>Patients and methods: </strong>Patients with R/M HNSCC were treated with niraparib and dostarlimab until disease progression or unacceptable toxicity. The primary endpoint was the overall response rate and clinical benefit assessed by RECIST version 1.1. Using Simon's two-step minimax design, 14 patients were planned to enroll in the first stage with a goal of overall clinical benefit of 50%.</p><p><strong>Results: </strong>Ten patients were enrolled. The majority were White males with a median age of 62.5. One patient had a PD-L1 combined positive score >20, a high tumor mutational burden, a BRCA1 rearrangement, and an ATRX splice site mutation. Nine patients previously failed anti-PD-1/PD-L1 therapy. The best overall response rate was 10%, with a 20% clinical benefit (1 partial response, 1 stable disease). The trial was terminated early for futility as the goal clinical benefit could not be reached. At a median follow-up of 10.13 months, the median progression-free survival was 3.8 months, and the median overall survival was 10.1 months. The most common grade 3 or higher treatment-related adverse events were thrombocytopenia and hypertension.</p><p><strong>Conclusions: </strong>The combination of niraparib and dostarlimab did not achieve the primary endpoint of clinical benefit, but activity may be improved with biomarker-driven treatment and selected patients.</p><p><strong>Significance: </strong>Patients with R/M HNSCC that progress on PD-1 inhibitors have poor prognoses. PARPis cause ssDNA breaks that accumulate in cells with mutations in DNA damage repair pathways, leading to synthetic lethality. However, PARPi also inhibits glycogen synthase kinase-3β activity, leading to upregulated PD-L1, which is abrogated by PD-1 inhibitors. In this study, we combine niraparib (PARPi) with dostarlimab (anti-PD-L1) to evaluate clinical benefit in patients with R/M HNSCC.</p>\",\"PeriodicalId\":72516,\"journal\":{\"name\":\"Cancer research communications\",\"volume\":\" \",\"pages\":\"939-944\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12146980/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer research communications\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1158/2767-9764.CRC-25-0192\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer research communications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1158/2767-9764.CRC-25-0192","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Phase II Study Evaluating the Efficacy of Niraparib and Dostarlimab (TSR-042) in Patients with Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma.
Purpose: Recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC) portends a poor prognosis. DNA pathway repair mutations in HNSCC are associated with higher tumor mutational burden rates and immune checkpoint inhibitor response. PARP inhibitors (PARPi) induce ssDNA breaks and are efficacious in cancers with DNA repair defects. Thus, we designed a single-arm, open-label, phase II clinical trial to evaluate the combination of niraparib and dostarlimab in patients with R/M HNSCC.
Patients and methods: Patients with R/M HNSCC were treated with niraparib and dostarlimab until disease progression or unacceptable toxicity. The primary endpoint was the overall response rate and clinical benefit assessed by RECIST version 1.1. Using Simon's two-step minimax design, 14 patients were planned to enroll in the first stage with a goal of overall clinical benefit of 50%.
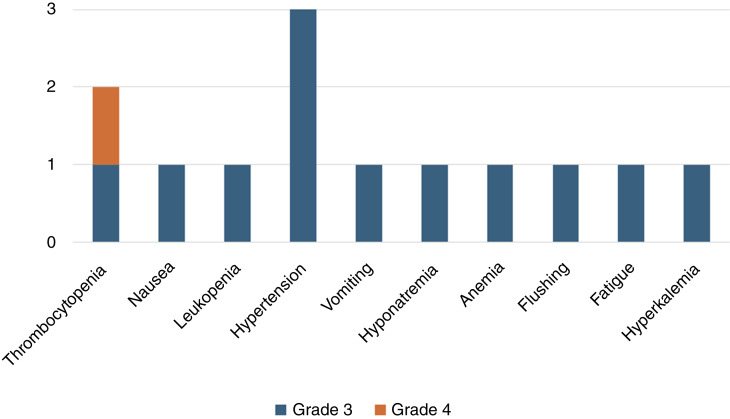
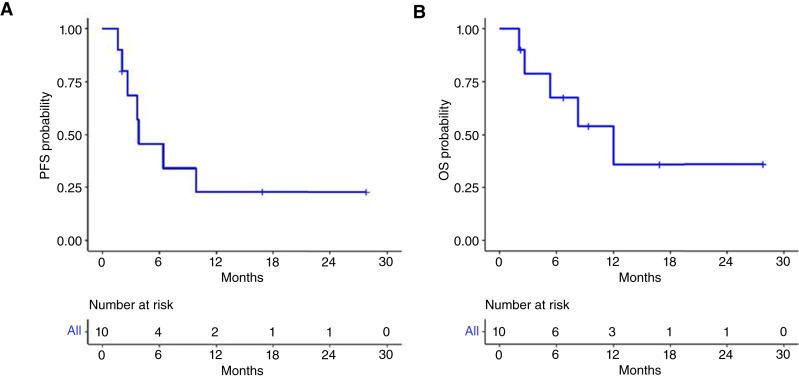
Results: Ten patients were enrolled. The majority were White males with a median age of 62.5. One patient had a PD-L1 combined positive score >20, a high tumor mutational burden, a BRCA1 rearrangement, and an ATRX splice site mutation. Nine patients previously failed anti-PD-1/PD-L1 therapy. The best overall response rate was 10%, with a 20% clinical benefit (1 partial response, 1 stable disease). The trial was terminated early for futility as the goal clinical benefit could not be reached. At a median follow-up of 10.13 months, the median progression-free survival was 3.8 months, and the median overall survival was 10.1 months. The most common grade 3 or higher treatment-related adverse events were thrombocytopenia and hypertension.
Conclusions: The combination of niraparib and dostarlimab did not achieve the primary endpoint of clinical benefit, but activity may be improved with biomarker-driven treatment and selected patients.
Significance: Patients with R/M HNSCC that progress on PD-1 inhibitors have poor prognoses. PARPis cause ssDNA breaks that accumulate in cells with mutations in DNA damage repair pathways, leading to synthetic lethality. However, PARPi also inhibits glycogen synthase kinase-3β activity, leading to upregulated PD-L1, which is abrogated by PD-1 inhibitors. In this study, we combine niraparib (PARPi) with dostarlimab (anti-PD-L1) to evaluate clinical benefit in patients with R/M HNSCC.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


