Radwa Fawzy Ahmed, Paul Fenton, Adityanarayan Bhatnagar, Victoria Wood, Andrew Bates
{"title":"在英国临床实践中,在根治性放化疗后对III期非小细胞肺癌实施辅助免疫治疗- PACIFIC试验结果在现实世界中可以实现吗?","authors":"Radwa Fawzy Ahmed, Paul Fenton, Adityanarayan Bhatnagar, Victoria Wood, Andrew Bates","doi":"10.1093/immadv/ltaf011","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>PACIFIC trial demonstrates improved progression-free survival (PFS) and overall survival (OS) in patients with locally advanced non-small-cell lung cancer (NSCLC) treated with platinum-based concurrent chemoradiotherapy (CRT) and adjuvant Durvalumab immunotherapy.</p><p><strong>Methods: </strong>We retrospectively reviewed 72 consecutive patients with locally advanced NSCLC treated with platinum-based concurrent CRT, who were potentially eligible for adjuvant Durvaluamb treatment (PDL1 ≥1% or inadequate). We analysed PFS, OS, treatment toxicity, and the impact of PDL1 on these outcomes.</p><p><strong>Results: </strong>The cohort median follow-up was 20 months. Fifty-five patients received adjuvant Durvalumab. The median OS (mOS) has not been reached. OS at 24 months was 67.8% for patients received Durvalumab. The median PFS (mPFS) for patients received Durvalumab was 30 months. PDL1 status (1-49% vs. ≥50%) did not affect outcome in our cohort. Sixteen patients stopped Durvalumab due to immune toxicity. At 24 months, 49% of these patients were still alive versus 76% of the patients who completed 12 months of treatment. The mOS for patients who stopped Durvalumab due to immune toxicity was 16 months, <i>P</i> = .0032. Seventeen patients did not receive adjuvant treatment due to insufficient performance status following CRT and mOS was 6 months.</p><p><strong>Conclusions: </strong>Our real-world experience demonstrates possibility to achieve similar outcomes to PACIFIC trial. PDL1 status did not affect clinical outcome in our cohort. Patients who stopped adjuvant Durvalumab treatment due to toxicity and those who were not deemed suitable to proceed with adjuvant Durvalumab after CRT, had poorer outcomes. This indicates that careful case selection remains essential.</p>","PeriodicalId":73353,"journal":{"name":"Immunotherapy advances","volume":"5 1","pages":"ltaf011"},"PeriodicalIF":4.9000,"publicationDate":"2025-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076069/pdf/","citationCount":"0","resultStr":"{\"title\":\"Implementing adjuvant immunotherapy following radical chemoradiotherapy for stage III non-small-cell lung cancer in UK clinical practice-Are the PACIFIC trial outcomes achievable in the real world?\",\"authors\":\"Radwa Fawzy Ahmed, Paul Fenton, Adityanarayan Bhatnagar, Victoria Wood, Andrew Bates\",\"doi\":\"10.1093/immadv/ltaf011\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>PACIFIC trial demonstrates improved progression-free survival (PFS) and overall survival (OS) in patients with locally advanced non-small-cell lung cancer (NSCLC) treated with platinum-based concurrent chemoradiotherapy (CRT) and adjuvant Durvalumab immunotherapy.</p><p><strong>Methods: </strong>We retrospectively reviewed 72 consecutive patients with locally advanced NSCLC treated with platinum-based concurrent CRT, who were potentially eligible for adjuvant Durvaluamb treatment (PDL1 ≥1% or inadequate). We analysed PFS, OS, treatment toxicity, and the impact of PDL1 on these outcomes.</p><p><strong>Results: </strong>The cohort median follow-up was 20 months. Fifty-five patients received adjuvant Durvalumab. The median OS (mOS) has not been reached. OS at 24 months was 67.8% for patients received Durvalumab. The median PFS (mPFS) for patients received Durvalumab was 30 months. PDL1 status (1-49% vs. ≥50%) did not affect outcome in our cohort. Sixteen patients stopped Durvalumab due to immune toxicity. At 24 months, 49% of these patients were still alive versus 76% of the patients who completed 12 months of treatment. The mOS for patients who stopped Durvalumab due to immune toxicity was 16 months, <i>P</i> = .0032. Seventeen patients did not receive adjuvant treatment due to insufficient performance status following CRT and mOS was 6 months.</p><p><strong>Conclusions: </strong>Our real-world experience demonstrates possibility to achieve similar outcomes to PACIFIC trial. PDL1 status did not affect clinical outcome in our cohort. Patients who stopped adjuvant Durvalumab treatment due to toxicity and those who were not deemed suitable to proceed with adjuvant Durvalumab after CRT, had poorer outcomes. This indicates that careful case selection remains essential.</p>\",\"PeriodicalId\":73353,\"journal\":{\"name\":\"Immunotherapy advances\",\"volume\":\"5 1\",\"pages\":\"ltaf011\"},\"PeriodicalIF\":4.9000,\"publicationDate\":\"2025-03-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076069/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Immunotherapy advances\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/immadv/ltaf011\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Immunotherapy advances","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/immadv/ltaf011","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Implementing adjuvant immunotherapy following radical chemoradiotherapy for stage III non-small-cell lung cancer in UK clinical practice-Are the PACIFIC trial outcomes achievable in the real world?
Introduction: PACIFIC trial demonstrates improved progression-free survival (PFS) and overall survival (OS) in patients with locally advanced non-small-cell lung cancer (NSCLC) treated with platinum-based concurrent chemoradiotherapy (CRT) and adjuvant Durvalumab immunotherapy.
Methods: We retrospectively reviewed 72 consecutive patients with locally advanced NSCLC treated with platinum-based concurrent CRT, who were potentially eligible for adjuvant Durvaluamb treatment (PDL1 ≥1% or inadequate). We analysed PFS, OS, treatment toxicity, and the impact of PDL1 on these outcomes.
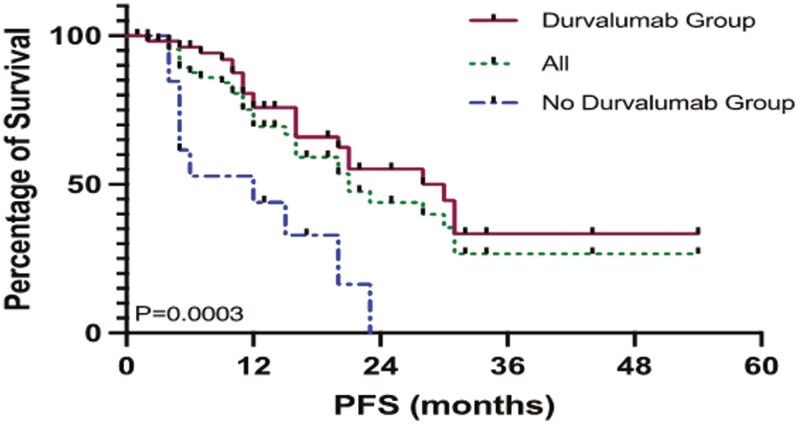
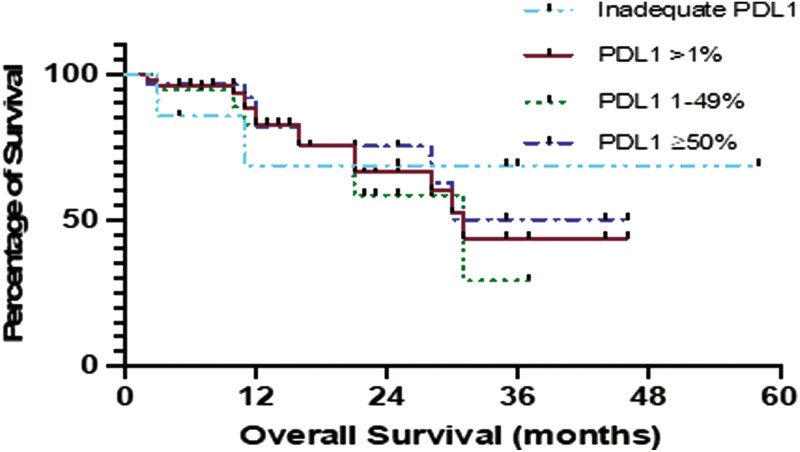
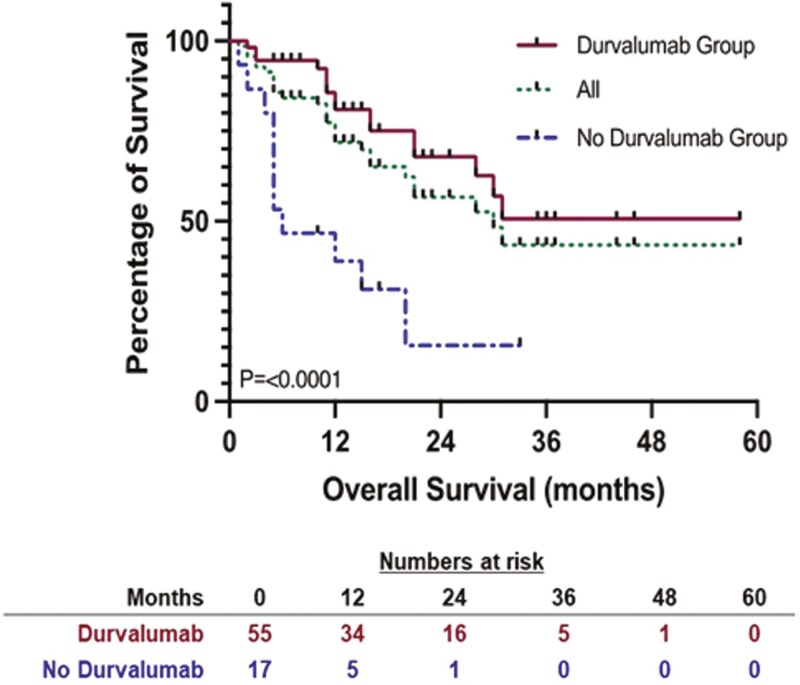
Results: The cohort median follow-up was 20 months. Fifty-five patients received adjuvant Durvalumab. The median OS (mOS) has not been reached. OS at 24 months was 67.8% for patients received Durvalumab. The median PFS (mPFS) for patients received Durvalumab was 30 months. PDL1 status (1-49% vs. ≥50%) did not affect outcome in our cohort. Sixteen patients stopped Durvalumab due to immune toxicity. At 24 months, 49% of these patients were still alive versus 76% of the patients who completed 12 months of treatment. The mOS for patients who stopped Durvalumab due to immune toxicity was 16 months, P = .0032. Seventeen patients did not receive adjuvant treatment due to insufficient performance status following CRT and mOS was 6 months.
Conclusions: Our real-world experience demonstrates possibility to achieve similar outcomes to PACIFIC trial. PDL1 status did not affect clinical outcome in our cohort. Patients who stopped adjuvant Durvalumab treatment due to toxicity and those who were not deemed suitable to proceed with adjuvant Durvalumab after CRT, had poorer outcomes. This indicates that careful case selection remains essential.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


