Eva-Corina Caragounis, Monika Fagevik Olsén, Lena Sandström, Rauni Rossi Norrlund, Lovisa Strömmer, Hans Granhed
{"title":"一项双机构观察性研究,比较临床和放射学连枷胸损伤的手术和非手术治疗的短期和长期结果。","authors":"Eva-Corina Caragounis, Monika Fagevik Olsén, Lena Sandström, Rauni Rossi Norrlund, Lovisa Strömmer, Hans Granhed","doi":"10.1186/s13049-025-01400-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Operative management of chest wall injuries requiring ventilatory support has been shown to decrease the time spent on ventilator. The main purpose of this study was to investigate whether operative management reduces the need for mechanical ventilation and the impact of surgery on long-term outcome concerning pain, lung function and movement.</p><p><strong>Methods: </strong>This is a bi-institutional prospective observational study comparing operative (Op) and non-operative (Non-Op) management of adult trauma patients with flail chest injuries. Data on the need for and LOS in intensive care (ICU), on mechanical ventilator (MV), and in hospital, and incidence of pneumonia and tracheostomy was collected. Clinical follow-up after six weeks, six months and one year concerning lung function, CT-lung volume, physical function, pain, and quality of life (QoL) was performed.</p><p><strong>Results: </strong>There was no difference in the need for (29%) and LOS on MV and in ICU between the Op and Non-Op groups. Chest wall surgery was performed 4 days (range 2-14) post trauma and associated with a longer hospital LOS. Pneumonia was more common in the Non-Op group (37% vs. 18%, p = 0.003). Fifty patients in the Op group and 38 patients in the Non-Op group were enrolled in a follow-up where Non-Op group experienced more pain in the first six months and had a higher daily dose of oral morphine during the first six weeks post trauma. The best residual lung function and CT-lung volume was seen in patients managed with muscle-sparing surgery without thoracotomy. No considerable difference in pain, physical activity, physical function and QoL were seen between the groups after one year.</p><p><strong>Conclusions: </strong>Operative management of flail chest injuries did not decrease the need for mechanical ventilation or the length of stay in ICU. Operating on non-ventilated patients may increase the length of hospital stay depending on day of surgery. Surgery was associated with a decreased incidence of pneumonia, less pain and subjective symptoms the first months' post-trauma despite operated patients being older and with more severe trauma, but after one year there were no significant differences between the groups. Operative technique may influence outcome and should be studied further.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov: NCT02132416, 7 May 2014.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"87"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082970/pdf/","citationCount":"0","resultStr":"{\"title\":\"A bi-institutional observational study comparing short-term and long-term outcome of operative and non-operative management of clinical and radiological flail chest injuries.\",\"authors\":\"Eva-Corina Caragounis, Monika Fagevik Olsén, Lena Sandström, Rauni Rossi Norrlund, Lovisa Strömmer, Hans Granhed\",\"doi\":\"10.1186/s13049-025-01400-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Operative management of chest wall injuries requiring ventilatory support has been shown to decrease the time spent on ventilator. The main purpose of this study was to investigate whether operative management reduces the need for mechanical ventilation and the impact of surgery on long-term outcome concerning pain, lung function and movement.</p><p><strong>Methods: </strong>This is a bi-institutional prospective observational study comparing operative (Op) and non-operative (Non-Op) management of adult trauma patients with flail chest injuries. Data on the need for and LOS in intensive care (ICU), on mechanical ventilator (MV), and in hospital, and incidence of pneumonia and tracheostomy was collected. Clinical follow-up after six weeks, six months and one year concerning lung function, CT-lung volume, physical function, pain, and quality of life (QoL) was performed.</p><p><strong>Results: </strong>There was no difference in the need for (29%) and LOS on MV and in ICU between the Op and Non-Op groups. Chest wall surgery was performed 4 days (range 2-14) post trauma and associated with a longer hospital LOS. Pneumonia was more common in the Non-Op group (37% vs. 18%, p = 0.003). Fifty patients in the Op group and 38 patients in the Non-Op group were enrolled in a follow-up where Non-Op group experienced more pain in the first six months and had a higher daily dose of oral morphine during the first six weeks post trauma. The best residual lung function and CT-lung volume was seen in patients managed with muscle-sparing surgery without thoracotomy. No considerable difference in pain, physical activity, physical function and QoL were seen between the groups after one year.</p><p><strong>Conclusions: </strong>Operative management of flail chest injuries did not decrease the need for mechanical ventilation or the length of stay in ICU. Operating on non-ventilated patients may increase the length of hospital stay depending on day of surgery. Surgery was associated with a decreased incidence of pneumonia, less pain and subjective symptoms the first months' post-trauma despite operated patients being older and with more severe trauma, but after one year there were no significant differences between the groups. Operative technique may influence outcome and should be studied further.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov: NCT02132416, 7 May 2014.</p>\",\"PeriodicalId\":49292,\"journal\":{\"name\":\"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine\",\"volume\":\"33 1\",\"pages\":\"87\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-05-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082970/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13049-025-01400-8\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01400-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:对需要呼吸机支持的胸壁损伤进行手术治疗可以减少使用呼吸机的时间。本研究的主要目的是探讨手术治疗是否减少了机械通气的需求,以及手术对疼痛、肺功能和运动等长期预后的影响。方法:这是一项双机构前瞻性观察研究,比较成人创伤患者连枷胸损伤的手术(Op)和非手术(Non-Op)治疗。收集重症监护室(ICU)、机械呼吸机(MV)和住院患者的需求和LOS以及肺炎和气管切开术的发生率的数据。临床随访6周、6个月和1年后肺功能、ct -肺容量、身体功能、疼痛和生活质量(QoL)。结果:手术组和非手术组在MV和ICU的LOS需求(29%)和LOS需求无差异。胸壁手术在创伤后4天(范围2-14天)进行,与较长的住院LOS相关。肺炎在非手术组更为常见(37% vs. 18%, p = 0.003)。手术组的50名患者和非手术组的38名患者参加了随访,在创伤后的前六个月,非手术组经历了更多的疼痛,并且在创伤后的前六周内,每天口服吗啡的剂量更高。保留肌肉手术而不开胸的患者的残余肺功能和ct肺容量最好。一年后,两组在疼痛、身体活动、身体功能和生活质量方面均无显著差异。结论:连枷胸损伤的手术处理并没有减少机械通气的需要或在ICU的住院时间。对非通气患者进行手术可能会增加住院时间,具体取决于手术日期。尽管手术患者年龄较大,创伤更严重,但在创伤后的头几个月,手术与肺炎发病率降低、疼痛和主观症状减轻有关,但一年后,两组之间没有显著差异。手术技术可能影响预后,应进一步研究。试验注册:ClinicalTrials.gov: nct02132416,2014年5月7日。
A bi-institutional observational study comparing short-term and long-term outcome of operative and non-operative management of clinical and radiological flail chest injuries.
Background: Operative management of chest wall injuries requiring ventilatory support has been shown to decrease the time spent on ventilator. The main purpose of this study was to investigate whether operative management reduces the need for mechanical ventilation and the impact of surgery on long-term outcome concerning pain, lung function and movement.
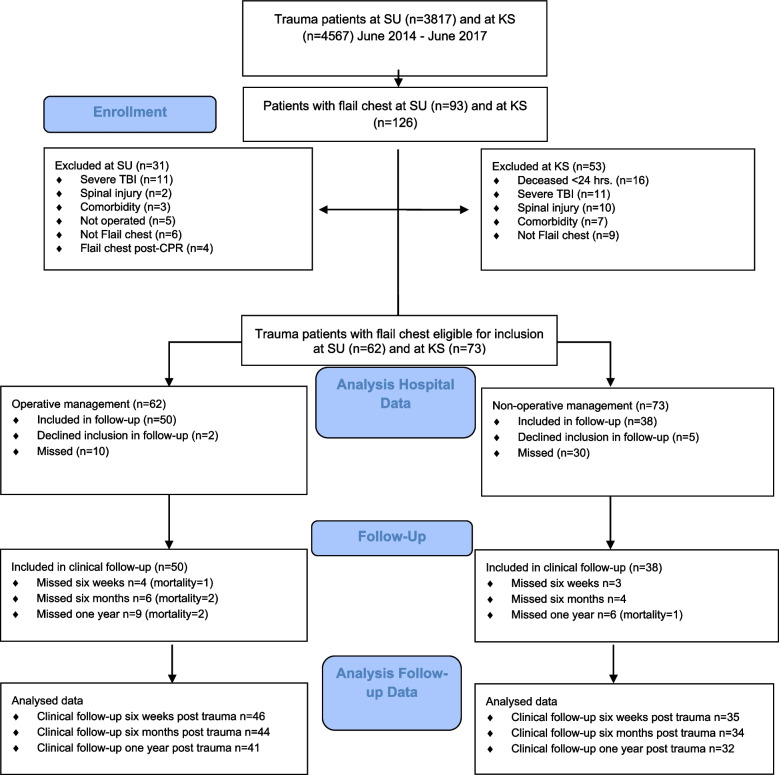
Methods: This is a bi-institutional prospective observational study comparing operative (Op) and non-operative (Non-Op) management of adult trauma patients with flail chest injuries. Data on the need for and LOS in intensive care (ICU), on mechanical ventilator (MV), and in hospital, and incidence of pneumonia and tracheostomy was collected. Clinical follow-up after six weeks, six months and one year concerning lung function, CT-lung volume, physical function, pain, and quality of life (QoL) was performed.
Results: There was no difference in the need for (29%) and LOS on MV and in ICU between the Op and Non-Op groups. Chest wall surgery was performed 4 days (range 2-14) post trauma and associated with a longer hospital LOS. Pneumonia was more common in the Non-Op group (37% vs. 18%, p = 0.003). Fifty patients in the Op group and 38 patients in the Non-Op group were enrolled in a follow-up where Non-Op group experienced more pain in the first six months and had a higher daily dose of oral morphine during the first six weeks post trauma. The best residual lung function and CT-lung volume was seen in patients managed with muscle-sparing surgery without thoracotomy. No considerable difference in pain, physical activity, physical function and QoL were seen between the groups after one year.
Conclusions: Operative management of flail chest injuries did not decrease the need for mechanical ventilation or the length of stay in ICU. Operating on non-ventilated patients may increase the length of hospital stay depending on day of surgery. Surgery was associated with a decreased incidence of pneumonia, less pain and subjective symptoms the first months' post-trauma despite operated patients being older and with more severe trauma, but after one year there were no significant differences between the groups. Operative technique may influence outcome and should be studied further.
Trial registration: ClinicalTrials.gov: NCT02132416, 7 May 2014.
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


