Simon Tournemine, Sylvie Bonvalot, Jean-Yves Mary, Dimosthenis Andreou, David Biau
{"title":"评价新辅助化疗对四肢软组织肉瘤可切除性的影响。","authors":"Simon Tournemine, Sylvie Bonvalot, Jean-Yves Mary, Dimosthenis Andreou, David Biau","doi":"10.1302/2633-1462.65.BJO-2025-0026.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>In this study, we explore whether neoadjuvant chemotherapy influences the surgical resection strategy devised by surgeons for high-grade soft-tissue sarcoma.</p><p><strong>Methods: </strong>A total of 12 experienced soft-tissue sarcoma surgeons rated patients who underwent neoadjuvant chemotherapy for a soft-tissue sarcoma of the thigh. Cases were randomly assigned to surgeons, such that each surgeon rated three out of the 12 cases, and each case was rated by three out of 12 surgeons (n = 36 ratings before and after chemotherapy). Surgeons were asked which surgical technique they would use: amputation; and if not, resection or dissection of critical anatomical structures in close proximity to the tumour (sciatic nerve, femoral artery, and femur). Pre- and post-chemotherapy ratings were then compared to test if chemotherapy changed the surgery aggressiveness anticipated by the surgeons.</p><p><strong>Results: </strong>Tumour volume increased in 9/12 cases (75%). Ratings as amputation were discordant in 5/36 cases (14%) before and after chemotherapy. The surgical technique planned by surgeons before and after chemotherapy regarding critical anatomical structures were discordant in five (14%), eight (22%), and six of 36 ratings (17%) for the sciatic nerve, the femoral artery, and the femur, respectively. Overall, a similarly aggressive surgery was planned by surgeons in nine, six, and eight cases for the sciatic nerve, the femoral artery, and the femur, respectively, which is significantly more than that expected due to chance alone. A more aggressive surgery was anticipated in five of 36 cases (14%).</p><p><strong>Conclusion: </strong>Despite tumour growth being observed in 75% of cases, the surgical resection strategy devised after neoadjuvant chemotherapy remained notably similar to the one devised prior to neoadjuvant chemotherapy for critical anatomical structures. However, 'switchers', namely patients identified as being at risk of needing an amputation if the tumour experiences slight growth, should undergo conservative surgery initially, followed by chemotherapy.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 5","pages":"553-559"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12081119/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of the effect of neoadjuvant chemotherapy on the planned resectability of extremity soft-tissue sarcomas.\",\"authors\":\"Simon Tournemine, Sylvie Bonvalot, Jean-Yves Mary, Dimosthenis Andreou, David Biau\",\"doi\":\"10.1302/2633-1462.65.BJO-2025-0026.R1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>In this study, we explore whether neoadjuvant chemotherapy influences the surgical resection strategy devised by surgeons for high-grade soft-tissue sarcoma.</p><p><strong>Methods: </strong>A total of 12 experienced soft-tissue sarcoma surgeons rated patients who underwent neoadjuvant chemotherapy for a soft-tissue sarcoma of the thigh. Cases were randomly assigned to surgeons, such that each surgeon rated three out of the 12 cases, and each case was rated by three out of 12 surgeons (n = 36 ratings before and after chemotherapy). Surgeons were asked which surgical technique they would use: amputation; and if not, resection or dissection of critical anatomical structures in close proximity to the tumour (sciatic nerve, femoral artery, and femur). Pre- and post-chemotherapy ratings were then compared to test if chemotherapy changed the surgery aggressiveness anticipated by the surgeons.</p><p><strong>Results: </strong>Tumour volume increased in 9/12 cases (75%). Ratings as amputation were discordant in 5/36 cases (14%) before and after chemotherapy. The surgical technique planned by surgeons before and after chemotherapy regarding critical anatomical structures were discordant in five (14%), eight (22%), and six of 36 ratings (17%) for the sciatic nerve, the femoral artery, and the femur, respectively. Overall, a similarly aggressive surgery was planned by surgeons in nine, six, and eight cases for the sciatic nerve, the femoral artery, and the femur, respectively, which is significantly more than that expected due to chance alone. A more aggressive surgery was anticipated in five of 36 cases (14%).</p><p><strong>Conclusion: </strong>Despite tumour growth being observed in 75% of cases, the surgical resection strategy devised after neoadjuvant chemotherapy remained notably similar to the one devised prior to neoadjuvant chemotherapy for critical anatomical structures. However, 'switchers', namely patients identified as being at risk of needing an amputation if the tumour experiences slight growth, should undergo conservative surgery initially, followed by chemotherapy.</p>\",\"PeriodicalId\":34103,\"journal\":{\"name\":\"Bone & Joint Open\",\"volume\":\"6 5\",\"pages\":\"553-559\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-05-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12081119/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bone & Joint Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1302/2633-1462.65.BJO-2025-0026.R1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.65.BJO-2025-0026.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Evaluation of the effect of neoadjuvant chemotherapy on the planned resectability of extremity soft-tissue sarcomas.
Aims: In this study, we explore whether neoadjuvant chemotherapy influences the surgical resection strategy devised by surgeons for high-grade soft-tissue sarcoma.
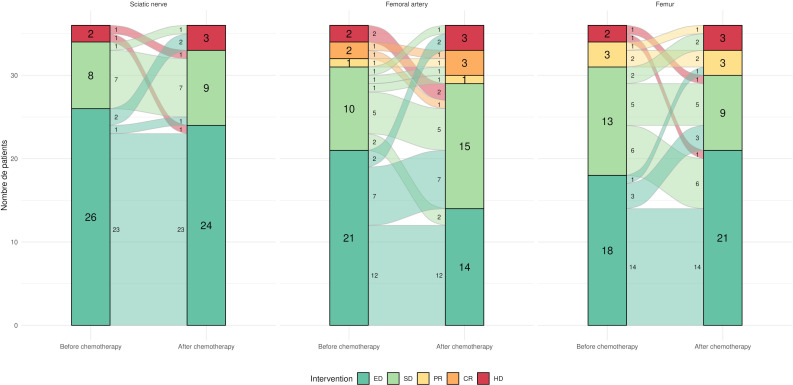
Methods: A total of 12 experienced soft-tissue sarcoma surgeons rated patients who underwent neoadjuvant chemotherapy for a soft-tissue sarcoma of the thigh. Cases were randomly assigned to surgeons, such that each surgeon rated three out of the 12 cases, and each case was rated by three out of 12 surgeons (n = 36 ratings before and after chemotherapy). Surgeons were asked which surgical technique they would use: amputation; and if not, resection or dissection of critical anatomical structures in close proximity to the tumour (sciatic nerve, femoral artery, and femur). Pre- and post-chemotherapy ratings were then compared to test if chemotherapy changed the surgery aggressiveness anticipated by the surgeons.
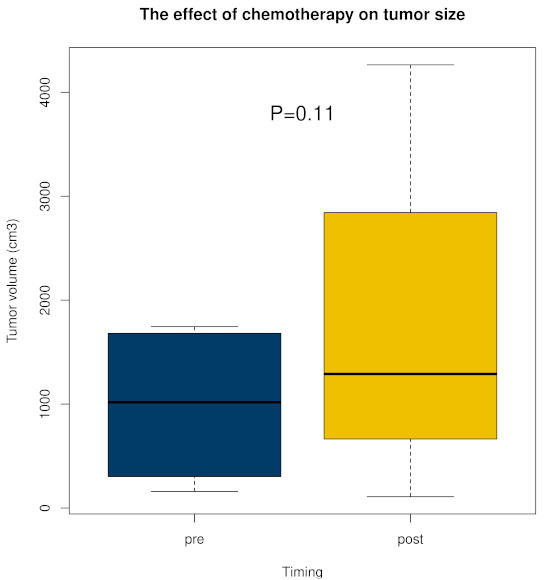
Results: Tumour volume increased in 9/12 cases (75%). Ratings as amputation were discordant in 5/36 cases (14%) before and after chemotherapy. The surgical technique planned by surgeons before and after chemotherapy regarding critical anatomical structures were discordant in five (14%), eight (22%), and six of 36 ratings (17%) for the sciatic nerve, the femoral artery, and the femur, respectively. Overall, a similarly aggressive surgery was planned by surgeons in nine, six, and eight cases for the sciatic nerve, the femoral artery, and the femur, respectively, which is significantly more than that expected due to chance alone. A more aggressive surgery was anticipated in five of 36 cases (14%).
Conclusion: Despite tumour growth being observed in 75% of cases, the surgical resection strategy devised after neoadjuvant chemotherapy remained notably similar to the one devised prior to neoadjuvant chemotherapy for critical anatomical structures. However, 'switchers', namely patients identified as being at risk of needing an amputation if the tumour experiences slight growth, should undergo conservative surgery initially, followed by chemotherapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


