Mark V Koning, Lassima Reijnen, Femy Kemperman, Eugenie Schipper-Reintjes
{"title":"手工稀释持续肾替代治疗液治疗无尿严重低钠血症患者:一例报告和系统评价。","authors":"Mark V Koning, Lassima Reijnen, Femy Kemperman, Eugenie Schipper-Reintjes","doi":"10.1159/000543718","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>When a patient with severe hyponatremia requires renal replacement therapy, a too rapid correction of sodium levels may occur. Manual dilution of the fluids during continuous renal replacement therapy (CRRT) is a method that can lead to a controlled correction of sodium. We present a case and add a systematic review to determine the feasibility of this method.</p><p><strong>Case presentation: </strong>A female was admitted to the intensive care unit with acute kidney failure due to anti-glomerular basement membrane antibody glomerulonephritis, anuria, and an initial sodium level of 100 mmol/L. She received CRRT with manually diluted fluids for 6 days, in which sodium levels increased from 108 mmol/L to 130 mmol/L. A search in Medline, Web of Science, and Google Scholar was added for the systematic review. The search yielded 49 cases, including the current report, of which 47 were anuric or oliguric, in which the fluids were diluted to a median of 8 mmol/L (interquartile range 5-11) (range 0-17) above the serum sodium, the median CRRT dose was 27 mL/kg/h (22-30) (13-77.5). This led to an increase in serum sodium of 0.2 mmol/L/h (0.1-0.3) (0-0.7).</p><p><strong>Conclusion: </strong>CRRT with manually diluted fluids in patients with severe hyponatremia and anuria can lead to a controlled increase serum sodium, while allowing sufficient RRT dose and fluid removal. Still, errors in dilution may occur and we recommend 4 hourly monitoring of serum sodium levels to timely detect an inadvertent increase in sodium.</p>","PeriodicalId":9599,"journal":{"name":"Case Reports in Nephrology and Dialysis","volume":"15 1","pages":"26-32"},"PeriodicalIF":0.9000,"publicationDate":"2025-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11857161/pdf/","citationCount":"0","resultStr":"{\"title\":\"Manual Dilution of Continuous Renal Replacement Therapy Fluids in Anuric Patients with Severe Hyponatremia: A Case Report and Systematic Review.\",\"authors\":\"Mark V Koning, Lassima Reijnen, Femy Kemperman, Eugenie Schipper-Reintjes\",\"doi\":\"10.1159/000543718\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>When a patient with severe hyponatremia requires renal replacement therapy, a too rapid correction of sodium levels may occur. Manual dilution of the fluids during continuous renal replacement therapy (CRRT) is a method that can lead to a controlled correction of sodium. We present a case and add a systematic review to determine the feasibility of this method.</p><p><strong>Case presentation: </strong>A female was admitted to the intensive care unit with acute kidney failure due to anti-glomerular basement membrane antibody glomerulonephritis, anuria, and an initial sodium level of 100 mmol/L. She received CRRT with manually diluted fluids for 6 days, in which sodium levels increased from 108 mmol/L to 130 mmol/L. A search in Medline, Web of Science, and Google Scholar was added for the systematic review. The search yielded 49 cases, including the current report, of which 47 were anuric or oliguric, in which the fluids were diluted to a median of 8 mmol/L (interquartile range 5-11) (range 0-17) above the serum sodium, the median CRRT dose was 27 mL/kg/h (22-30) (13-77.5). This led to an increase in serum sodium of 0.2 mmol/L/h (0.1-0.3) (0-0.7).</p><p><strong>Conclusion: </strong>CRRT with manually diluted fluids in patients with severe hyponatremia and anuria can lead to a controlled increase serum sodium, while allowing sufficient RRT dose and fluid removal. Still, errors in dilution may occur and we recommend 4 hourly monitoring of serum sodium levels to timely detect an inadvertent increase in sodium.</p>\",\"PeriodicalId\":9599,\"journal\":{\"name\":\"Case Reports in Nephrology and Dialysis\",\"volume\":\"15 1\",\"pages\":\"26-32\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-01-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11857161/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Nephrology and Dialysis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000543718\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology and Dialysis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000543718","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
当严重低钠血症患者需要肾脏替代治疗时,可能会出现过快的钠水平纠正。在持续肾替代治疗(CRRT)期间,人工稀释液体是一种可导致钠控制校正的方法。我们提出了一个案例,并增加了一个系统的审查,以确定该方法的可行性。病例介绍:一名女性因抗肾小球基底膜抗体肾小球肾炎,无尿,初始钠水平为100 mmol/L而急性肾衰竭住进重症监护室。患者接受人工稀释液体CRRT治疗6天,钠水平从108 mmol/L增加到130 mmol/L。在Medline, Web of Science和b谷歌Scholar中进行了搜索,以进行系统评价。包括本报告在内的49例中,47例无尿或少尿,其中液体被稀释至高于血清钠的中位数8 mmol/L(四分位数范围5-11)(范围0-17),中位CRRT剂量为27 mL/kg/h(22-30)(13-77.5)。这导致血清钠升高0.2 mmol/L/h(0.1-0.3)(0-0.7)。结论:严重低钠血症和无尿患者手工稀释液体CRRT可控制血清钠的增加,同时允许足够的RRT剂量和液体排出。尽管如此,稀释可能会出现错误,我们建议每4小时监测血清钠水平,以及时发现钠的无意增加。
Manual Dilution of Continuous Renal Replacement Therapy Fluids in Anuric Patients with Severe Hyponatremia: A Case Report and Systematic Review.
Introduction: When a patient with severe hyponatremia requires renal replacement therapy, a too rapid correction of sodium levels may occur. Manual dilution of the fluids during continuous renal replacement therapy (CRRT) is a method that can lead to a controlled correction of sodium. We present a case and add a systematic review to determine the feasibility of this method.
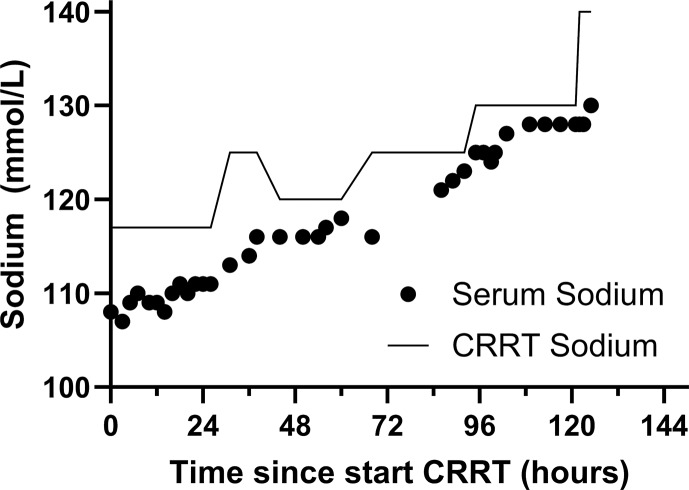
Case presentation: A female was admitted to the intensive care unit with acute kidney failure due to anti-glomerular basement membrane antibody glomerulonephritis, anuria, and an initial sodium level of 100 mmol/L. She received CRRT with manually diluted fluids for 6 days, in which sodium levels increased from 108 mmol/L to 130 mmol/L. A search in Medline, Web of Science, and Google Scholar was added for the systematic review. The search yielded 49 cases, including the current report, of which 47 were anuric or oliguric, in which the fluids were diluted to a median of 8 mmol/L (interquartile range 5-11) (range 0-17) above the serum sodium, the median CRRT dose was 27 mL/kg/h (22-30) (13-77.5). This led to an increase in serum sodium of 0.2 mmol/L/h (0.1-0.3) (0-0.7).
Conclusion: CRRT with manually diluted fluids in patients with severe hyponatremia and anuria can lead to a controlled increase serum sodium, while allowing sufficient RRT dose and fluid removal. Still, errors in dilution may occur and we recommend 4 hourly monitoring of serum sodium levels to timely detect an inadvertent increase in sodium.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of nephrology and dialysis, including genetic susceptibility, clinical presentation, diagnosis, treatment or prevention, toxicities of therapy, critical care, supportive care, quality-of-life and survival issues. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


