Amal Haujir, Michael Tøstesen, Tarec Christoffer El-Galaly, Thomas Stauffer Larsen, Jørn Starklint, Christian Bjørn Poulsen, Pär Lars Josefsson, Erik Clasen-Linde, Michael Pedersen, Andriette Dessau-Arp, Michael Roost Clausen, Judit Mészáros Jørgensen
{"title":"利妥昔单抗和生物仿制药利妥昔单抗治疗未经治疗的弥漫性大b细胞淋巴瘤的有效性,丹麦基于人群的分析。","authors":"Amal Haujir, Michael Tøstesen, Tarec Christoffer El-Galaly, Thomas Stauffer Larsen, Jørn Starklint, Christian Bjørn Poulsen, Pär Lars Josefsson, Erik Clasen-Linde, Michael Pedersen, Andriette Dessau-Arp, Michael Roost Clausen, Judit Mészáros Jørgensen","doi":"10.1111/bjh.20155","DOIUrl":null,"url":null,"abstract":"<p>Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of malignant lymphoma. The annual incidence in Denmark is about 450 cases comparable to other western countries.<span><sup>1</sup></span> Conventional chemotherapy, for example CHOP (cyclophosphamide, hydroxydaunorubicin, vincristine and prednisone), has for five decades been the standard treatment of DLBCL.<span><sup>2</sup></span> Rituximab, a monoclonal anti-CD20 antibody drug, was introduced around the year 2000 after positive phase 3 studies in DLBCL.<span><sup>3</sup></span> Around 2015, the patent of rituximab ended, and biosimilar products were developed. Antibodies are complex molecules consisting of large, folded polypeptide molecules. There is a risk of variation between the molecules, for example due to post-translational modifications. However, the effect of biosimilar rituximab is intended to be identical to generic rituximab. Upon entering the market, the new biosimilar anti-CD20 antibodies (Ritemvia, Rixathon and Ruxience) have been tested in clinical trials against rituximab.<span><sup>4-7</sup></span> However, limited data exist on the performance of biosimilar anti-CD20 antibodies in real-world populations.</p><p>We aimed to assess the efficacy of biosimilar rituximab compared to rituximab on progression-free survival (PFS), defined as either registered relapse or death from any cause, and overall survival (OS) in Danish patients with previously untreated DLBCL.</p><p>Patients with DLBCL diagnosed between January 2015 and January 2022 were identified in the population-based lymphoma registry in Denmark, LYFO.<span><sup>8</sup></span> Inclusion criteria were a first-time diagnosis of DLBCL, treatment with R-CHOP or R-CHOP-like regimens (R-CEOP [cyclophosphamide, etoposide, vincristine and prednisone], R-CHOEP [cyclophosphamide, hydroxydaunorubicin, vincristine, etoposide and prednisone], R-COPE [cyclophosphamide, vincristine, etoposide and prednisone] or R-CHIC [combination of CHOP and CHOEP]). Patients with primary central nervous system lymphoma and missing data on treatment were excluded. The main other regimen than CHOP was R-CHOEP, which comprised 71% in the CHOP-like category. In a recent publication, also based on data from LYFO, outcomes were comparable to standard R-CHOP.<span><sup>9</sup></span></p><p>Patients were stratified according to treatment with rituximab or biosimilar rituximab. From the pharmacies of the treating hospitals, we gathered information on the exact date of change to biosimilar rituximab.</p><p>To evaluate outcomes, we used the Kaplan–Meier method and Cox regression analysis. The multivariable model was adjusted for International Prognostic Index factors, sex and age. The proportional hazards assumption was evaluated graphically using log minus log plots. Analyses were conducted using Stata/IC 14.2 (Stata Statistical Software: Release 14. StataCorp LP: College Station, TX). The study was compliant with national regulations concerning registry-based research.</p><p>We identified 2.372 eligible patients diagnosed with DLBCL between January 2015 and January 2022. They were predominantly males with a median age of 70 years (range: 18–95 years). The median age was 69 years for 1.137 patients treated with rituximab and 71 years for 1.235 patients treated with biosimilar rituximab. The proportion of female patients was 40.7%. No clinically meaningful differences in baseline characteristics were observed (Table 1).</p><p>We observed comparable PFS and OS. The 3-year PFS was 71.8% (95% confidence interval [CI] 69.1–74.3) and 72.2% (95% CI 69.3–74.9) for patients treated with rituximab and biosimilar rituximab respectively (Figure 1). The 3-year OS was 77.5% (95% CI 74.9–79.8) and 76.9% (95% CI 74.1–79.4) respectively.</p><p>In the multivariable analysis, we found no difference in PFS or OS with a hazard ratio of 0.94 (95% CI 0.81–1.10) and 0.99 (95% CI 0.83–1.17) respectively (Figure 1).</p><p>In this study, we evaluated PFS and OS of biosimilar rituximab compared with rituximab in patients with newly diagnosed DLBCL using a national, population-based lymphoma registry in Denmark. The study did not show any difference in OS or PFS. Using nationwide validated data, we were able to identify possible confounders and adjust appropriately. The historical comparison of our two treatment groups occurred within a short time span, and the Danish national treatment guideline for DLBCL was unchanged during that time.</p><p>The median age was +2 years in the biosimilar group compared to the rituximab group. This may reflect an increasing willingness over time to offer chemotherapy to elderly patients. Elderly patients typically receive ‘other’ chemotherapy, most likely mini-CHOP. In the rituximab group, treated earlier in the inclusion period, a lower proportion of elderly patients received chemotherapy. Finally, the average age of the general population increased over the study period.</p><p>These results are in line with a previous European study.<span><sup>10</sup></span> However, in the latter, only OS was reported as an outcome. Improvement of salvage therapies and availability of clinical trials for relapsed/refractory patients in the later years might have improved the OS in the biosimilar group. For this reason, PFS might be a better end-point to assess the effect of biosimilar rituximab.</p><p>The main strength of this study is the use of a nationwide population-based lymphoma registry. This allowed for a large sample size. Additionally, the risk of selection bias is minimal due to tax-financed specialist care centralized in few centres. Lastly, uniform nationwide treatment guidelines ensure consistent management across centres. These results support the non-inferiority of biosimilar rituximab, reassuring that use is both safe and efficacious. This could make treatment accessible for more people and result in less economic stress on healthcare systems. These results substantiate the continued use of biosimilar rituximab in patients with DLBCL.</p><p>Amal Haujir, Michael Tøstesen, Tarec Christoffer El-Galaly, Thomas Stauffer Larsen, Jørn Starklint, Christian Bjørn Poulsen, Pär Lars Josefsson, Erik Clasen-Linde, Michael Pedersen, Andriette Dessau-Arp, Michael Roost Clausen, and Judit Mészáros Jørgensen all wrote the paper and provided the data possible for this study. Michael Roost Clausen analysed the data. Judit Mészáros Jørgensen designed the study.</p><p>No funding was received for this study.</p><p>The authors declare no conflicts of interest.</p><p>The study was registered at Region Syd, Denmark. Journal nr.: 21/53806.</p>","PeriodicalId":135,"journal":{"name":"British Journal of Haematology","volume":"207 1","pages":"270-272"},"PeriodicalIF":3.8000,"publicationDate":"2025-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bjh.20155","citationCount":"0","resultStr":"{\"title\":\"Effectiveness of rituximab and biosimilar rituximab in untreated diffuse large B-cell lymphoma, a Danish population-based analysis\",\"authors\":\"Amal Haujir, Michael Tøstesen, Tarec Christoffer El-Galaly, Thomas Stauffer Larsen, Jørn Starklint, Christian Bjørn Poulsen, Pär Lars Josefsson, Erik Clasen-Linde, Michael Pedersen, Andriette Dessau-Arp, Michael Roost Clausen, Judit Mészáros Jørgensen\",\"doi\":\"10.1111/bjh.20155\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of malignant lymphoma. The annual incidence in Denmark is about 450 cases comparable to other western countries.<span><sup>1</sup></span> Conventional chemotherapy, for example CHOP (cyclophosphamide, hydroxydaunorubicin, vincristine and prednisone), has for five decades been the standard treatment of DLBCL.<span><sup>2</sup></span> Rituximab, a monoclonal anti-CD20 antibody drug, was introduced around the year 2000 after positive phase 3 studies in DLBCL.<span><sup>3</sup></span> Around 2015, the patent of rituximab ended, and biosimilar products were developed. Antibodies are complex molecules consisting of large, folded polypeptide molecules. There is a risk of variation between the molecules, for example due to post-translational modifications. However, the effect of biosimilar rituximab is intended to be identical to generic rituximab. Upon entering the market, the new biosimilar anti-CD20 antibodies (Ritemvia, Rixathon and Ruxience) have been tested in clinical trials against rituximab.<span><sup>4-7</sup></span> However, limited data exist on the performance of biosimilar anti-CD20 antibodies in real-world populations.</p><p>We aimed to assess the efficacy of biosimilar rituximab compared to rituximab on progression-free survival (PFS), defined as either registered relapse or death from any cause, and overall survival (OS) in Danish patients with previously untreated DLBCL.</p><p>Patients with DLBCL diagnosed between January 2015 and January 2022 were identified in the population-based lymphoma registry in Denmark, LYFO.<span><sup>8</sup></span> Inclusion criteria were a first-time diagnosis of DLBCL, treatment with R-CHOP or R-CHOP-like regimens (R-CEOP [cyclophosphamide, etoposide, vincristine and prednisone], R-CHOEP [cyclophosphamide, hydroxydaunorubicin, vincristine, etoposide and prednisone], R-COPE [cyclophosphamide, vincristine, etoposide and prednisone] or R-CHIC [combination of CHOP and CHOEP]). Patients with primary central nervous system lymphoma and missing data on treatment were excluded. The main other regimen than CHOP was R-CHOEP, which comprised 71% in the CHOP-like category. In a recent publication, also based on data from LYFO, outcomes were comparable to standard R-CHOP.<span><sup>9</sup></span></p><p>Patients were stratified according to treatment with rituximab or biosimilar rituximab. From the pharmacies of the treating hospitals, we gathered information on the exact date of change to biosimilar rituximab.</p><p>To evaluate outcomes, we used the Kaplan–Meier method and Cox regression analysis. The multivariable model was adjusted for International Prognostic Index factors, sex and age. The proportional hazards assumption was evaluated graphically using log minus log plots. Analyses were conducted using Stata/IC 14.2 (Stata Statistical Software: Release 14. StataCorp LP: College Station, TX). The study was compliant with national regulations concerning registry-based research.</p><p>We identified 2.372 eligible patients diagnosed with DLBCL between January 2015 and January 2022. They were predominantly males with a median age of 70 years (range: 18–95 years). The median age was 69 years for 1.137 patients treated with rituximab and 71 years for 1.235 patients treated with biosimilar rituximab. The proportion of female patients was 40.7%. No clinically meaningful differences in baseline characteristics were observed (Table 1).</p><p>We observed comparable PFS and OS. The 3-year PFS was 71.8% (95% confidence interval [CI] 69.1–74.3) and 72.2% (95% CI 69.3–74.9) for patients treated with rituximab and biosimilar rituximab respectively (Figure 1). The 3-year OS was 77.5% (95% CI 74.9–79.8) and 76.9% (95% CI 74.1–79.4) respectively.</p><p>In the multivariable analysis, we found no difference in PFS or OS with a hazard ratio of 0.94 (95% CI 0.81–1.10) and 0.99 (95% CI 0.83–1.17) respectively (Figure 1).</p><p>In this study, we evaluated PFS and OS of biosimilar rituximab compared with rituximab in patients with newly diagnosed DLBCL using a national, population-based lymphoma registry in Denmark. The study did not show any difference in OS or PFS. Using nationwide validated data, we were able to identify possible confounders and adjust appropriately. The historical comparison of our two treatment groups occurred within a short time span, and the Danish national treatment guideline for DLBCL was unchanged during that time.</p><p>The median age was +2 years in the biosimilar group compared to the rituximab group. This may reflect an increasing willingness over time to offer chemotherapy to elderly patients. Elderly patients typically receive ‘other’ chemotherapy, most likely mini-CHOP. In the rituximab group, treated earlier in the inclusion period, a lower proportion of elderly patients received chemotherapy. Finally, the average age of the general population increased over the study period.</p><p>These results are in line with a previous European study.<span><sup>10</sup></span> However, in the latter, only OS was reported as an outcome. Improvement of salvage therapies and availability of clinical trials for relapsed/refractory patients in the later years might have improved the OS in the biosimilar group. For this reason, PFS might be a better end-point to assess the effect of biosimilar rituximab.</p><p>The main strength of this study is the use of a nationwide population-based lymphoma registry. This allowed for a large sample size. Additionally, the risk of selection bias is minimal due to tax-financed specialist care centralized in few centres. Lastly, uniform nationwide treatment guidelines ensure consistent management across centres. These results support the non-inferiority of biosimilar rituximab, reassuring that use is both safe and efficacious. This could make treatment accessible for more people and result in less economic stress on healthcare systems. These results substantiate the continued use of biosimilar rituximab in patients with DLBCL.</p><p>Amal Haujir, Michael Tøstesen, Tarec Christoffer El-Galaly, Thomas Stauffer Larsen, Jørn Starklint, Christian Bjørn Poulsen, Pär Lars Josefsson, Erik Clasen-Linde, Michael Pedersen, Andriette Dessau-Arp, Michael Roost Clausen, and Judit Mészáros Jørgensen all wrote the paper and provided the data possible for this study. Michael Roost Clausen analysed the data. Judit Mészáros Jørgensen designed the study.</p><p>No funding was received for this study.</p><p>The authors declare no conflicts of interest.</p><p>The study was registered at Region Syd, Denmark. Journal nr.: 21/53806.</p>\",\"PeriodicalId\":135,\"journal\":{\"name\":\"British Journal of Haematology\",\"volume\":\"207 1\",\"pages\":\"270-272\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-05-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bjh.20155\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"British Journal of Haematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/bjh.20155\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"British Journal of Haematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bjh.20155","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
弥漫性大b细胞淋巴瘤(DLBCL)是恶性淋巴瘤最常见的亚型。丹麦的年发病率约为450例,与其他西方国家相当传统化疗,如CHOP(环磷酰胺、羟基柔红霉素、长春新碱、强尼松),五十年来一直是dlbcl的标准治疗方案。2000年左右,dlbcl的三期研究呈阳性,抗cd20单克隆药物利妥昔单抗(Rituximab)被引入。3 2015年左右,利妥昔单抗专利结束,生物仿制药开发。抗体是由大的折叠多肽分子组成的复杂分子。分子之间存在变异的风险,例如由于翻译后修饰。然而,生物仿制药利妥昔单抗的效果与仿制药利妥昔单抗相同。进入市场后,新的生物类似药抗cd20抗体(Ritemvia, Rixathon和Ruxience)已经在针对利妥昔单抗的临床试验中进行了测试。然而,关于抗cd20生物类似药在真实人群中的表现的数据有限。我们的目的是评估生物仿制药利妥昔单抗与利妥昔单抗在丹麦未经治疗的DLBCL患者的无进展生存期(PFS)和总生存期(OS)方面的疗效,PFS定义为登记复发或任何原因死亡。在2015年1月至2022年1月期间诊断为DLBCL的患者在丹麦基于人群的淋巴瘤登记中被确定,纳入标准是首次诊断为DLBCL,接受R-CHOP或R-CHOP样方案(R-CEOP[环磷酰胺,依泊泊苷,长春新碱和泼尼松],R-CHOEP[环磷酰胺,羟基柔红霉素,长春新碱,依泊泊苷和泼尼松],R-COPE[环磷酰胺,长春新碱,依托泊苷和强的松]或R-CHIC [CHOP和CHOEP的组合])。排除原发性中枢神经系统淋巴瘤和治疗资料缺失的患者。CHOP之外的其他主要方案是R-CHOEP,占CHOP类方案的71%。在最近的一篇文章中,同样基于LYFO的数据,结果与标准R-CHOP相当。根据利妥昔单抗或利妥昔单抗生物类似药对患者进行分层。从治疗医院的药房,我们收集了改变为生物仿制药利妥昔单抗的确切日期的信息。为了评估结果,我们使用Kaplan-Meier方法和Cox回归分析。多变量模型根据国际预后指数因素、性别和年龄进行调整。比例风险假设用对数-对数图进行图形化评价。使用Stata/IC 14.2 (Stata Statistical Software: Release 14)进行分析。StataCorp LP: College Station, TX)。本研究符合国家关于登记研究的规定。我们在2015年1月至2022年1月期间确定了2.372例诊断为DLBCL的符合条件的患者。他们主要是男性,年龄中位数为70岁(范围:18-95岁)。接受利妥昔单抗治疗的1.137例患者中位年龄为69岁,接受利妥昔单抗生物仿制药治疗的1.235例患者中位年龄为71岁。女性患者占40.7%。基线特征没有观察到有临床意义的差异(表1)。我们观察到PFS和OS具有可比性。利妥昔单抗和生物类似药利妥昔单抗治疗的3年PFS分别为71.8%(95%置信区间[CI] 69.1-74.3)和72.2% (95% CI 69.3-74.9)(图1)。3年OS分别为77.5% (95% CI 74.9-79.8)和76.9% (95% CI 74.1-79.4)。在多变量分析中,我们发现PFS和OS无差异,风险比分别为0.94 (95% CI 0.81-1.10)和0.99 (95% CI 0.83-1.17)(图1)。在这项研究中,我们利用丹麦全国基于人群的淋巴瘤登记处评估了生物仿制药利妥昔单抗与利妥昔单抗在新诊断的DLBCL患者中的PFS和OS。该研究未显示OS或PFS有任何差异。使用全国范围内经过验证的数据,我们能够识别可能的混杂因素并进行适当调整。我们两个治疗组的历史比较发生在很短的时间跨度内,并且丹麦的DLBCL国家治疗指南在此期间没有变化。与利妥昔单抗组相比,生物仿制药组的中位年龄为+2岁。这可能反映出,随着时间的推移,人们越来越愿意为老年患者提供化疗。老年患者通常接受“其他”化疗,最有可能是mini-CHOP。在利妥昔单抗组中,在纳入期治疗较早,老年患者接受化疗的比例较低。最后,在研究期间,一般人群的平均年龄增加了。这些结果与之前欧洲的一项研究一致然而,在后者中,仅报告了OS作为结果。
Effectiveness of rituximab and biosimilar rituximab in untreated diffuse large B-cell lymphoma, a Danish population-based analysis
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of malignant lymphoma. The annual incidence in Denmark is about 450 cases comparable to other western countries.1 Conventional chemotherapy, for example CHOP (cyclophosphamide, hydroxydaunorubicin, vincristine and prednisone), has for five decades been the standard treatment of DLBCL.2 Rituximab, a monoclonal anti-CD20 antibody drug, was introduced around the year 2000 after positive phase 3 studies in DLBCL.3 Around 2015, the patent of rituximab ended, and biosimilar products were developed. Antibodies are complex molecules consisting of large, folded polypeptide molecules. There is a risk of variation between the molecules, for example due to post-translational modifications. However, the effect of biosimilar rituximab is intended to be identical to generic rituximab. Upon entering the market, the new biosimilar anti-CD20 antibodies (Ritemvia, Rixathon and Ruxience) have been tested in clinical trials against rituximab.4-7 However, limited data exist on the performance of biosimilar anti-CD20 antibodies in real-world populations.
We aimed to assess the efficacy of biosimilar rituximab compared to rituximab on progression-free survival (PFS), defined as either registered relapse or death from any cause, and overall survival (OS) in Danish patients with previously untreated DLBCL.
Patients with DLBCL diagnosed between January 2015 and January 2022 were identified in the population-based lymphoma registry in Denmark, LYFO.8 Inclusion criteria were a first-time diagnosis of DLBCL, treatment with R-CHOP or R-CHOP-like regimens (R-CEOP [cyclophosphamide, etoposide, vincristine and prednisone], R-CHOEP [cyclophosphamide, hydroxydaunorubicin, vincristine, etoposide and prednisone], R-COPE [cyclophosphamide, vincristine, etoposide and prednisone] or R-CHIC [combination of CHOP and CHOEP]). Patients with primary central nervous system lymphoma and missing data on treatment were excluded. The main other regimen than CHOP was R-CHOEP, which comprised 71% in the CHOP-like category. In a recent publication, also based on data from LYFO, outcomes were comparable to standard R-CHOP.9
Patients were stratified according to treatment with rituximab or biosimilar rituximab. From the pharmacies of the treating hospitals, we gathered information on the exact date of change to biosimilar rituximab.
To evaluate outcomes, we used the Kaplan–Meier method and Cox regression analysis. The multivariable model was adjusted for International Prognostic Index factors, sex and age. The proportional hazards assumption was evaluated graphically using log minus log plots. Analyses were conducted using Stata/IC 14.2 (Stata Statistical Software: Release 14. StataCorp LP: College Station, TX). The study was compliant with national regulations concerning registry-based research.
We identified 2.372 eligible patients diagnosed with DLBCL between January 2015 and January 2022. They were predominantly males with a median age of 70 years (range: 18–95 years). The median age was 69 years for 1.137 patients treated with rituximab and 71 years for 1.235 patients treated with biosimilar rituximab. The proportion of female patients was 40.7%. No clinically meaningful differences in baseline characteristics were observed (Table 1).
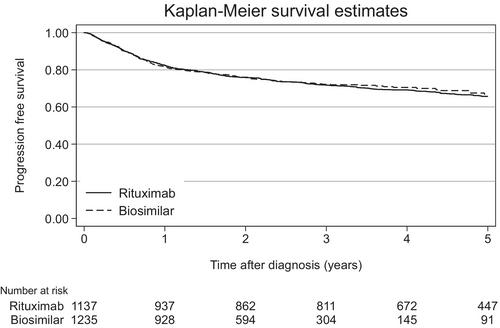
We observed comparable PFS and OS. The 3-year PFS was 71.8% (95% confidence interval [CI] 69.1–74.3) and 72.2% (95% CI 69.3–74.9) for patients treated with rituximab and biosimilar rituximab respectively (Figure 1). The 3-year OS was 77.5% (95% CI 74.9–79.8) and 76.9% (95% CI 74.1–79.4) respectively.
In the multivariable analysis, we found no difference in PFS or OS with a hazard ratio of 0.94 (95% CI 0.81–1.10) and 0.99 (95% CI 0.83–1.17) respectively (Figure 1).
In this study, we evaluated PFS and OS of biosimilar rituximab compared with rituximab in patients with newly diagnosed DLBCL using a national, population-based lymphoma registry in Denmark. The study did not show any difference in OS or PFS. Using nationwide validated data, we were able to identify possible confounders and adjust appropriately. The historical comparison of our two treatment groups occurred within a short time span, and the Danish national treatment guideline for DLBCL was unchanged during that time.
The median age was +2 years in the biosimilar group compared to the rituximab group. This may reflect an increasing willingness over time to offer chemotherapy to elderly patients. Elderly patients typically receive ‘other’ chemotherapy, most likely mini-CHOP. In the rituximab group, treated earlier in the inclusion period, a lower proportion of elderly patients received chemotherapy. Finally, the average age of the general population increased over the study period.
These results are in line with a previous European study.10 However, in the latter, only OS was reported as an outcome. Improvement of salvage therapies and availability of clinical trials for relapsed/refractory patients in the later years might have improved the OS in the biosimilar group. For this reason, PFS might be a better end-point to assess the effect of biosimilar rituximab.
The main strength of this study is the use of a nationwide population-based lymphoma registry. This allowed for a large sample size. Additionally, the risk of selection bias is minimal due to tax-financed specialist care centralized in few centres. Lastly, uniform nationwide treatment guidelines ensure consistent management across centres. These results support the non-inferiority of biosimilar rituximab, reassuring that use is both safe and efficacious. This could make treatment accessible for more people and result in less economic stress on healthcare systems. These results substantiate the continued use of biosimilar rituximab in patients with DLBCL.
Amal Haujir, Michael Tøstesen, Tarec Christoffer El-Galaly, Thomas Stauffer Larsen, Jørn Starklint, Christian Bjørn Poulsen, Pär Lars Josefsson, Erik Clasen-Linde, Michael Pedersen, Andriette Dessau-Arp, Michael Roost Clausen, and Judit Mészáros Jørgensen all wrote the paper and provided the data possible for this study. Michael Roost Clausen analysed the data. Judit Mészáros Jørgensen designed the study.
No funding was received for this study.
The authors declare no conflicts of interest.
The study was registered at Region Syd, Denmark. Journal nr.: 21/53806.
期刊介绍:
The British Journal of Haematology publishes original research papers in clinical, laboratory and experimental haematology. The Journal also features annotations, reviews, short reports, images in haematology and Letters to the Editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


