Shuang-Zheng Jia, Duan Yang, Xue-Jiao Yang, Rui Wang, Xi Yang, Man-Ni Huang, Ju-Sheng An
{"title":"淋巴结阳性早期宫颈癌根治性子宫切除术后放化疗的风险分层:一项回顾性单中心研究","authors":"Shuang-Zheng Jia, Duan Yang, Xue-Jiao Yang, Rui Wang, Xi Yang, Man-Ni Huang, Ju-Sheng An","doi":"10.1186/s13014-025-02655-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Limited data exist on the effectiveness of concurrent chemoradiotherapy (CRT) using intensity-modulated radiation therapy (IMRT) after radical surgery in patients with node-positive early-stage cervical cancer. This study aimed to identify prognostic factors and categorize patients into risk groups for personalized adjuvant therapy.</p><p><strong>Methods: </strong>The study included consecutive patients with pathologically confirmed node-positive cervical cancer who underwent radical hysterectomy and lymphadenectomy followed by CRT from January 2013 to October 2024 at our institute. Patients with parametrial invasion or positive resection margins were excluded. All patients received modern volumetric-modulated arc therapy with platinum-based concurrent chemotherapy. Data on clinicopathologic features, treatment details, and oncologic outcomes were collected. Univariate and multivariate Cox regression analyses were conducted to identify factors associated with disease-free survival (DFS) and overall survival (OS). Patients were further stratified into distinct risk categories for recurrence based on identified prognostic factors.</p><p><strong>Results: </strong>A total of 160 patients were included, with a median age of 44 years. The median number of lymph nodes retrieved was 33, and 11 patients presented with para-aortic lymph node metastasis (LNM). Over a median follow-up period of 39.7 months, 31 patients experienced disease progression, and 12 succumbed to the disease, yielding 3-year DFS and OS rates of 81.3% and 93.7%, respectively. Multivariate analysis identified non-squamous histotype (hazard ratio [HR]: 1.526, 95% confidence interval [CI]: 1.044-2.232, p = 0.029) and LNM ≥ 4 (HR: 1.521, 95% CI: 1.027-2.252, p = 0.036) as independent predictors of poorer DFS. Utilizing these prognostic factors for DFS, a risk stratification system was developed, categorizing patients into low-risk (no risk factors, n = 108) and high-intermediate risk (one or two risk factors, n = 52) groups. The high-intermediate-risk group exhibited significantly inferior DFS and OS compared to the low-risk group (3-year DFS: 67.4% versus 87.3%, HR: 1.697, 95% CI: 1.192-2.417, p = 0.002; 3-year OS: 82.5% versus 98.8%, HR: 3.577, 95% CI: 1.668-7.667, p < 0.001, respectively).</p><p><strong>Conclusions: </strong>Node-positive early-stage cervical cancer exhibits heterogeneous outcomes following radical hysterectomy and postoperative CRT. In patients with non-SCC histotype or ≥ 4 LNM, consolidation chemotherapy does not confer an additional survival benefit, indicating a need for innovative therapeutic strategies.</p>","PeriodicalId":49639,"journal":{"name":"Radiation Oncology","volume":"20 1","pages":"73"},"PeriodicalIF":3.3000,"publicationDate":"2025-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076833/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk stratification of node-positive early-stage cervical cancer treated with radical hysterectomy followed by chemoradiotherapy: a retrospective single-center study.\",\"authors\":\"Shuang-Zheng Jia, Duan Yang, Xue-Jiao Yang, Rui Wang, Xi Yang, Man-Ni Huang, Ju-Sheng An\",\"doi\":\"10.1186/s13014-025-02655-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Limited data exist on the effectiveness of concurrent chemoradiotherapy (CRT) using intensity-modulated radiation therapy (IMRT) after radical surgery in patients with node-positive early-stage cervical cancer. This study aimed to identify prognostic factors and categorize patients into risk groups for personalized adjuvant therapy.</p><p><strong>Methods: </strong>The study included consecutive patients with pathologically confirmed node-positive cervical cancer who underwent radical hysterectomy and lymphadenectomy followed by CRT from January 2013 to October 2024 at our institute. Patients with parametrial invasion or positive resection margins were excluded. All patients received modern volumetric-modulated arc therapy with platinum-based concurrent chemotherapy. Data on clinicopathologic features, treatment details, and oncologic outcomes were collected. Univariate and multivariate Cox regression analyses were conducted to identify factors associated with disease-free survival (DFS) and overall survival (OS). Patients were further stratified into distinct risk categories for recurrence based on identified prognostic factors.</p><p><strong>Results: </strong>A total of 160 patients were included, with a median age of 44 years. The median number of lymph nodes retrieved was 33, and 11 patients presented with para-aortic lymph node metastasis (LNM). Over a median follow-up period of 39.7 months, 31 patients experienced disease progression, and 12 succumbed to the disease, yielding 3-year DFS and OS rates of 81.3% and 93.7%, respectively. Multivariate analysis identified non-squamous histotype (hazard ratio [HR]: 1.526, 95% confidence interval [CI]: 1.044-2.232, p = 0.029) and LNM ≥ 4 (HR: 1.521, 95% CI: 1.027-2.252, p = 0.036) as independent predictors of poorer DFS. Utilizing these prognostic factors for DFS, a risk stratification system was developed, categorizing patients into low-risk (no risk factors, n = 108) and high-intermediate risk (one or two risk factors, n = 52) groups. The high-intermediate-risk group exhibited significantly inferior DFS and OS compared to the low-risk group (3-year DFS: 67.4% versus 87.3%, HR: 1.697, 95% CI: 1.192-2.417, p = 0.002; 3-year OS: 82.5% versus 98.8%, HR: 3.577, 95% CI: 1.668-7.667, p < 0.001, respectively).</p><p><strong>Conclusions: </strong>Node-positive early-stage cervical cancer exhibits heterogeneous outcomes following radical hysterectomy and postoperative CRT. In patients with non-SCC histotype or ≥ 4 LNM, consolidation chemotherapy does not confer an additional survival benefit, indicating a need for innovative therapeutic strategies.</p>\",\"PeriodicalId\":49639,\"journal\":{\"name\":\"Radiation Oncology\",\"volume\":\"20 1\",\"pages\":\"73\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2025-05-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076833/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiation Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13014-025-02655-2\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13014-025-02655-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:关于淋巴结阳性早期宫颈癌患者根治性手术后同步放化疗(CRT)使用调强放疗(IMRT)的有效性的数据有限。本研究旨在确定预后因素,并将患者分为危险组进行个性化辅助治疗。方法:本研究纳入2013年1月至2024年10月在我院连续行根治性子宫切除术和淋巴结切除术并行CRT的病理证实的淋巴结阳性宫颈癌患者。排除了参数性侵犯或切除边缘阳性的患者。所有患者均接受以铂为基础的同步化疗的现代体积调节弧治疗。收集了临床病理特征、治疗细节和肿瘤结果的数据。进行单因素和多因素Cox回归分析以确定与无病生存期(DFS)和总生存期(OS)相关的因素。根据确定的预后因素,将患者进一步分为不同的复发风险类别。结果:共纳入160例患者,中位年龄44岁。中位淋巴结数为33个,11例出现主动脉旁淋巴结转移(LNM)。在39.7个月的中位随访期间,31例患者出现疾病进展,12例患者死亡,3年DFS和OS率分别为81.3%和93.7%。多因素分析发现,非鳞状组织型(风险比[HR]: 1.526, 95%可信区间[CI]: 1.044-2.232, p = 0.029)和LNM≥4(风险比:1.521,95% CI: 1.027-2.252, p = 0.036)是较差DFS的独立预测因子。利用这些DFS的预后因素,建立了一个风险分层系统,将患者分为低危(无危险因素,n = 108)和中高危(一种或两种危险因素,n = 52)组。中高危组的DFS和OS明显低于低危组(3年DFS: 67.4% vs 87.3%, HR: 1.697, 95% CI: 1.192 ~ 2.417, p = 0.002;3年OS: 82.5% vs . 98.8%, HR: 3.577, 95% CI: 1.668-7.667, p结论:淋巴结阳性的早期宫颈癌在根治性子宫切除术和术后CRT后表现出异质性。对于非鳞状细胞癌组织型或≥4 LNM的患者,巩固化疗不能带来额外的生存益处,这表明需要创新的治疗策略。
Risk stratification of node-positive early-stage cervical cancer treated with radical hysterectomy followed by chemoradiotherapy: a retrospective single-center study.
Background: Limited data exist on the effectiveness of concurrent chemoradiotherapy (CRT) using intensity-modulated radiation therapy (IMRT) after radical surgery in patients with node-positive early-stage cervical cancer. This study aimed to identify prognostic factors and categorize patients into risk groups for personalized adjuvant therapy.
Methods: The study included consecutive patients with pathologically confirmed node-positive cervical cancer who underwent radical hysterectomy and lymphadenectomy followed by CRT from January 2013 to October 2024 at our institute. Patients with parametrial invasion or positive resection margins were excluded. All patients received modern volumetric-modulated arc therapy with platinum-based concurrent chemotherapy. Data on clinicopathologic features, treatment details, and oncologic outcomes were collected. Univariate and multivariate Cox regression analyses were conducted to identify factors associated with disease-free survival (DFS) and overall survival (OS). Patients were further stratified into distinct risk categories for recurrence based on identified prognostic factors.
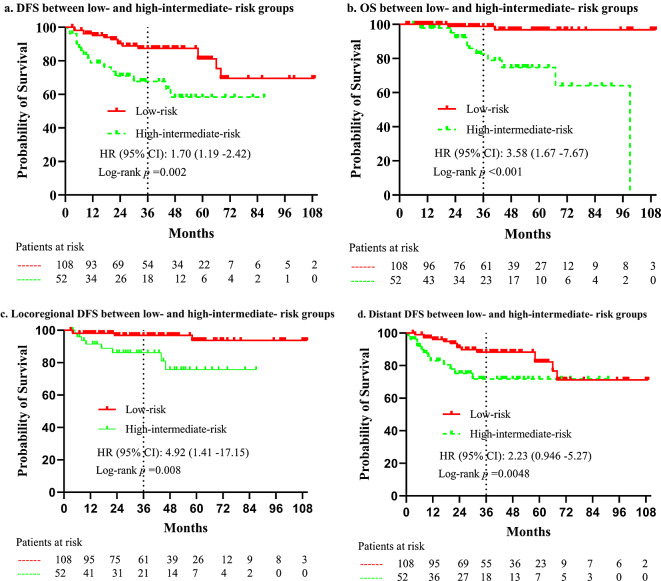
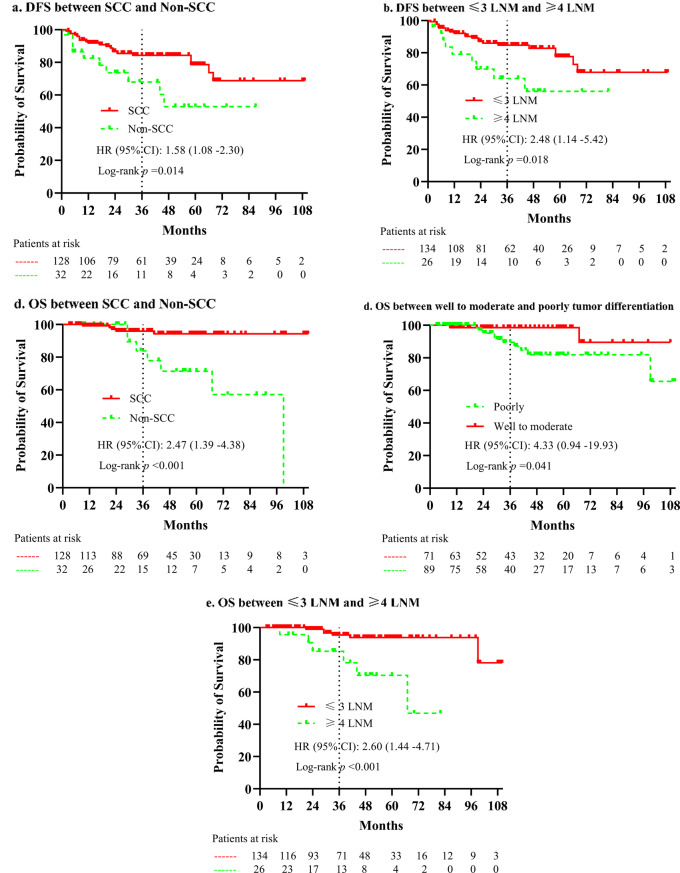
Results: A total of 160 patients were included, with a median age of 44 years. The median number of lymph nodes retrieved was 33, and 11 patients presented with para-aortic lymph node metastasis (LNM). Over a median follow-up period of 39.7 months, 31 patients experienced disease progression, and 12 succumbed to the disease, yielding 3-year DFS and OS rates of 81.3% and 93.7%, respectively. Multivariate analysis identified non-squamous histotype (hazard ratio [HR]: 1.526, 95% confidence interval [CI]: 1.044-2.232, p = 0.029) and LNM ≥ 4 (HR: 1.521, 95% CI: 1.027-2.252, p = 0.036) as independent predictors of poorer DFS. Utilizing these prognostic factors for DFS, a risk stratification system was developed, categorizing patients into low-risk (no risk factors, n = 108) and high-intermediate risk (one or two risk factors, n = 52) groups. The high-intermediate-risk group exhibited significantly inferior DFS and OS compared to the low-risk group (3-year DFS: 67.4% versus 87.3%, HR: 1.697, 95% CI: 1.192-2.417, p = 0.002; 3-year OS: 82.5% versus 98.8%, HR: 3.577, 95% CI: 1.668-7.667, p < 0.001, respectively).
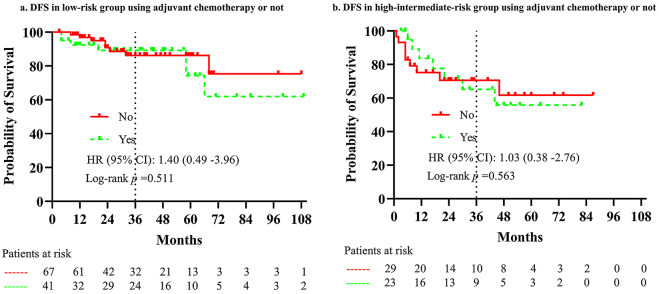
Conclusions: Node-positive early-stage cervical cancer exhibits heterogeneous outcomes following radical hysterectomy and postoperative CRT. In patients with non-SCC histotype or ≥ 4 LNM, consolidation chemotherapy does not confer an additional survival benefit, indicating a need for innovative therapeutic strategies.
Radiation OncologyONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
6.50
自引率
2.80%
发文量
181
审稿时长
3-6 weeks
期刊介绍:
Radiation Oncology encompasses all aspects of research that impacts on the treatment of cancer using radiation. It publishes findings in molecular and cellular radiation biology, radiation physics, radiation technology, and clinical oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


