Bård Uleberg, Kaare Harald Bønaa, Kari Krizak Halle, Bjarne K Jacobsen, Beate Hauglann, Eva Stensland, Olav Helge Førde
{"title":"延迟再灌注治疗与st段抬高型心肌梗死患者左室射血分数降低的关系:一项全国前瞻性队列研究。","authors":"Bård Uleberg, Kaare Harald Bønaa, Kari Krizak Halle, Bjarne K Jacobsen, Beate Hauglann, Eva Stensland, Olav Helge Førde","doi":"10.1093/ehjopen/oeaf034","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The aim of this nationwide study of patients with acute ST-segment elevation myocardial infarction (STEMI) was to investigate the relation between delayed reperfusion and mildly to moderately reduced and severely reduced left ventricular ejection fraction (LVEF).</p><p><strong>Methods and results: </strong>In this national population-based cohort study, log-binominal and modified Poisson regression models were applied to examine the associations between delayed reperfusion (i.e. fibrinolysis > 30 min or primary percutaneous coronary intervention > 120 min after first medical contact) and reduced LVEF, adjusted for reperfusion strategy, and patient characteristics. A total of 6567 Norwegian patients with STEMI registered in the Norwegian Registry of Myocardial Infarction during 2015-2018 were included in the analyses. Among them, 57% had normal LVEF (≥50%), 39% had mildly to moderately reduced LVEF (31-49%), and 4% had severely reduced LVEF (≤30%), measured during the acute admission. The adjusted relative risk of having a mildly to moderately reduced LVEF was 1.11 [95% confidence interval (CI) 1.04-1.18] for patients receiving delayed vs. timely reperfusion, and the adjusted relative risk of having severely reduced LVEF was 1.76 (95% CI 1.37-2.25) for patients receiving delayed vs. timely reperfusion. Reperfusion strategy, either primary percutaneous coronary intervention (pPCI) or a pharmacoinvasive strategy (PI), was not a significant determinant for reduced LVEF in any of the analyses.</p><p><strong>Conclusion: </strong>Delayed reperfusion treatment in STEMI increases the risk of mildly to moderately reduced LVEF, and the risk of severely reduced LVEF substantially, compared with timely reperfusion. The risk of reduced LVEF did not differ between patients treated with pPCI or PI.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 2","pages":"oeaf034"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12001758/pdf/","citationCount":"0","resultStr":"{\"title\":\"The relation between delayed reperfusion treatment and reduced left ventricular ejection fraction in patients with ST-segment elevation myocardial infarction: a national prospective cohort study.\",\"authors\":\"Bård Uleberg, Kaare Harald Bønaa, Kari Krizak Halle, Bjarne K Jacobsen, Beate Hauglann, Eva Stensland, Olav Helge Førde\",\"doi\":\"10.1093/ehjopen/oeaf034\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The aim of this nationwide study of patients with acute ST-segment elevation myocardial infarction (STEMI) was to investigate the relation between delayed reperfusion and mildly to moderately reduced and severely reduced left ventricular ejection fraction (LVEF).</p><p><strong>Methods and results: </strong>In this national population-based cohort study, log-binominal and modified Poisson regression models were applied to examine the associations between delayed reperfusion (i.e. fibrinolysis > 30 min or primary percutaneous coronary intervention > 120 min after first medical contact) and reduced LVEF, adjusted for reperfusion strategy, and patient characteristics. A total of 6567 Norwegian patients with STEMI registered in the Norwegian Registry of Myocardial Infarction during 2015-2018 were included in the analyses. Among them, 57% had normal LVEF (≥50%), 39% had mildly to moderately reduced LVEF (31-49%), and 4% had severely reduced LVEF (≤30%), measured during the acute admission. The adjusted relative risk of having a mildly to moderately reduced LVEF was 1.11 [95% confidence interval (CI) 1.04-1.18] for patients receiving delayed vs. timely reperfusion, and the adjusted relative risk of having severely reduced LVEF was 1.76 (95% CI 1.37-2.25) for patients receiving delayed vs. timely reperfusion. Reperfusion strategy, either primary percutaneous coronary intervention (pPCI) or a pharmacoinvasive strategy (PI), was not a significant determinant for reduced LVEF in any of the analyses.</p><p><strong>Conclusion: </strong>Delayed reperfusion treatment in STEMI increases the risk of mildly to moderately reduced LVEF, and the risk of severely reduced LVEF substantially, compared with timely reperfusion. The risk of reduced LVEF did not differ between patients treated with pPCI or PI.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 2\",\"pages\":\"oeaf034\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-04-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12001758/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf034\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf034","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:这项全国性的急性st段抬高型心肌梗死(STEMI)患者研究的目的是探讨延迟再灌注与轻度至中度降低和严重降低左心室射血分数(LVEF)之间的关系。方法和结果:在这项以全国人群为基础的队列研究中,应用对数二项和修正泊松回归模型来检验延迟再灌注(即首次医疗接触后30分钟纤维蛋白溶解>或首次经皮冠状动脉介入> 120分钟)与LVEF降低之间的关系,并根据再灌注策略和患者特征进行调整。2015-2018年期间在挪威心肌梗死登记处登记的6567名STEMI挪威患者被纳入分析。其中57%的患者在急性入院时LVEF正常(≥50%),39%的患者LVEF轻度至中度降低(31-49%),4%的患者LVEF严重降低(≤30%)。延迟再灌注与及时再灌注患者LVEF轻度至中度降低的校正相对风险为1.11[95%置信区间(CI) 1.04-1.18],延迟再灌注与及时再灌注患者LVEF严重降低的校正相对风险为1.76 (95% CI 1.37-2.25)。再灌注策略,无论是初级经皮冠状动脉介入治疗(pPCI)还是药物侵入策略(PI),在任何分析中都不是降低LVEF的重要决定因素。结论:与及时再灌注相比,STEMI延迟再灌注治疗使LVEF轻度至中度降低的风险显著增加,严重LVEF降低的风险显著增加。在接受pPCI或PI治疗的患者中,LVEF降低的风险没有差异。
The relation between delayed reperfusion treatment and reduced left ventricular ejection fraction in patients with ST-segment elevation myocardial infarction: a national prospective cohort study.
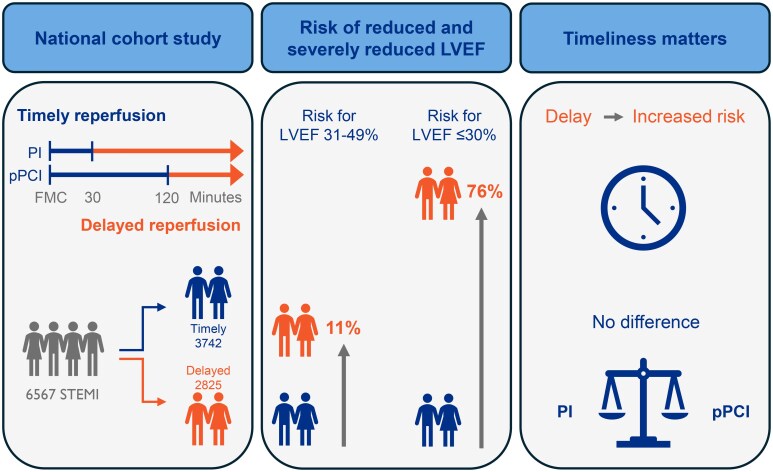
Aims: The aim of this nationwide study of patients with acute ST-segment elevation myocardial infarction (STEMI) was to investigate the relation between delayed reperfusion and mildly to moderately reduced and severely reduced left ventricular ejection fraction (LVEF).
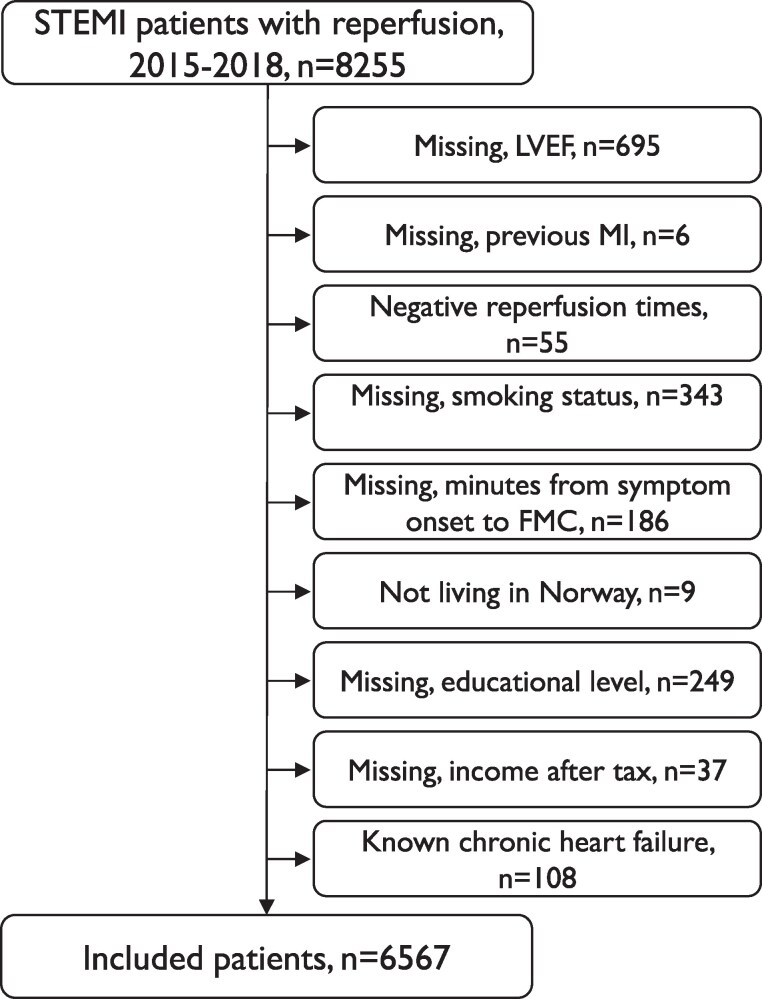
Methods and results: In this national population-based cohort study, log-binominal and modified Poisson regression models were applied to examine the associations between delayed reperfusion (i.e. fibrinolysis > 30 min or primary percutaneous coronary intervention > 120 min after first medical contact) and reduced LVEF, adjusted for reperfusion strategy, and patient characteristics. A total of 6567 Norwegian patients with STEMI registered in the Norwegian Registry of Myocardial Infarction during 2015-2018 were included in the analyses. Among them, 57% had normal LVEF (≥50%), 39% had mildly to moderately reduced LVEF (31-49%), and 4% had severely reduced LVEF (≤30%), measured during the acute admission. The adjusted relative risk of having a mildly to moderately reduced LVEF was 1.11 [95% confidence interval (CI) 1.04-1.18] for patients receiving delayed vs. timely reperfusion, and the adjusted relative risk of having severely reduced LVEF was 1.76 (95% CI 1.37-2.25) for patients receiving delayed vs. timely reperfusion. Reperfusion strategy, either primary percutaneous coronary intervention (pPCI) or a pharmacoinvasive strategy (PI), was not a significant determinant for reduced LVEF in any of the analyses.
Conclusion: Delayed reperfusion treatment in STEMI increases the risk of mildly to moderately reduced LVEF, and the risk of severely reduced LVEF substantially, compared with timely reperfusion. The risk of reduced LVEF did not differ between patients treated with pPCI or PI.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


