Catherine R Marinac, Charles H McDonnell, Lincoln D Nadauld, Christina A Dilaveri, Robert Reid, Karen C Chung, Margarita Lopatin, Eric T Fung, Deborah Schrag, Rita Shaknovich, Eric A Klein
{"title":"在PATHFINDER研究中,多种癌症早期检测测试对癌症信号起源预测和诊断解决的临床评价。","authors":"Catherine R Marinac, Charles H McDonnell, Lincoln D Nadauld, Christina A Dilaveri, Robert Reid, Karen C Chung, Margarita Lopatin, Eric T Fung, Deborah Schrag, Rita Shaknovich, Eric A Klein","doi":"10.1158/1940-6207.CAPR-24-0468","DOIUrl":null,"url":null,"abstract":"<p><p>Blood-based multicancer early detection (MCED) tests represent a new approach for cancer detection. To gain insights into the utility of various approaches of evaluating a cancer signal detected (CSD) test result, we evaluated diagnostic journeys of a subset of 6,662 participants in PATHFINDER who had a CSD on both an initial and refined version of an MCED test that also provided a prediction of cancer signal origin (CSO). We sought to determine whether CSO prediction-guided diagnostic evaluations led to diagnostic resolution; whether participants with known risk factors for cancer beyond age alone and a negative initial diagnostic evaluation had a cancer diagnosis during study follow-up; the utility of whole-body imaging in reaching diagnostic resolution; and differences in the diagnostic journeys needed to reach diagnostic resolution for both true- and false-positive results. Of the 39 participants in this analysis, 82% (32/39) achieved diagnostic resolution after the initial evaluation, including 78% (25/32) who reached resolution specifically with a CSO prediction-directed workup. Eighteen percent (7/39) required additional evaluation for persistent clinical suspicion of cancer, all of whom achieved resolution (3 with and 4 without cancer). Whole-body imaging contributed to diagnostic resolution in only 49% of CSD cases. Approximately 90% of true- and false-positive cases had imaging tests; more true positives versus false positives (81.0% vs. 38.9%) had nonsurgical and/or surgical procedures. In conclusion, CSO prediction-directed evaluations enabled diagnostic resolution for most participants, although some with negative initial evaluations but persistent suspicion of cancer required additional testing.</p><p><strong>Prevention relevance: </strong>MCED testing has the potential to increase detection of cancer at earlier stages. As MCED testing is a new technology, there are few data on the diagnostic journeys patients undergo following testing. We observed that for most patients, CSO prediction-directed workups were efficient, leading to diagnostic resolution after initial evaluation.</p>","PeriodicalId":72514,"journal":{"name":"Cancer prevention research (Philadelphia, Pa.)","volume":" ","pages":"475-483"},"PeriodicalIF":2.6000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314506/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Evaluation of Cancer Signal Origin Prediction and Diagnostic Resolution following Multicancer Early Detection Testing in the PATHFINDER Study.\",\"authors\":\"Catherine R Marinac, Charles H McDonnell, Lincoln D Nadauld, Christina A Dilaveri, Robert Reid, Karen C Chung, Margarita Lopatin, Eric T Fung, Deborah Schrag, Rita Shaknovich, Eric A Klein\",\"doi\":\"10.1158/1940-6207.CAPR-24-0468\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Blood-based multicancer early detection (MCED) tests represent a new approach for cancer detection. To gain insights into the utility of various approaches of evaluating a cancer signal detected (CSD) test result, we evaluated diagnostic journeys of a subset of 6,662 participants in PATHFINDER who had a CSD on both an initial and refined version of an MCED test that also provided a prediction of cancer signal origin (CSO). We sought to determine whether CSO prediction-guided diagnostic evaluations led to diagnostic resolution; whether participants with known risk factors for cancer beyond age alone and a negative initial diagnostic evaluation had a cancer diagnosis during study follow-up; the utility of whole-body imaging in reaching diagnostic resolution; and differences in the diagnostic journeys needed to reach diagnostic resolution for both true- and false-positive results. Of the 39 participants in this analysis, 82% (32/39) achieved diagnostic resolution after the initial evaluation, including 78% (25/32) who reached resolution specifically with a CSO prediction-directed workup. Eighteen percent (7/39) required additional evaluation for persistent clinical suspicion of cancer, all of whom achieved resolution (3 with and 4 without cancer). Whole-body imaging contributed to diagnostic resolution in only 49% of CSD cases. Approximately 90% of true- and false-positive cases had imaging tests; more true positives versus false positives (81.0% vs. 38.9%) had nonsurgical and/or surgical procedures. In conclusion, CSO prediction-directed evaluations enabled diagnostic resolution for most participants, although some with negative initial evaluations but persistent suspicion of cancer required additional testing.</p><p><strong>Prevention relevance: </strong>MCED testing has the potential to increase detection of cancer at earlier stages. As MCED testing is a new technology, there are few data on the diagnostic journeys patients undergo following testing. We observed that for most patients, CSO prediction-directed workups were efficient, leading to diagnostic resolution after initial evaluation.</p>\",\"PeriodicalId\":72514,\"journal\":{\"name\":\"Cancer prevention research (Philadelphia, Pa.)\",\"volume\":\" \",\"pages\":\"475-483\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314506/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer prevention research (Philadelphia, Pa.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1158/1940-6207.CAPR-24-0468\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer prevention research (Philadelphia, Pa.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1158/1940-6207.CAPR-24-0468","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Clinical Evaluation of Cancer Signal Origin Prediction and Diagnostic Resolution following Multicancer Early Detection Testing in the PATHFINDER Study.
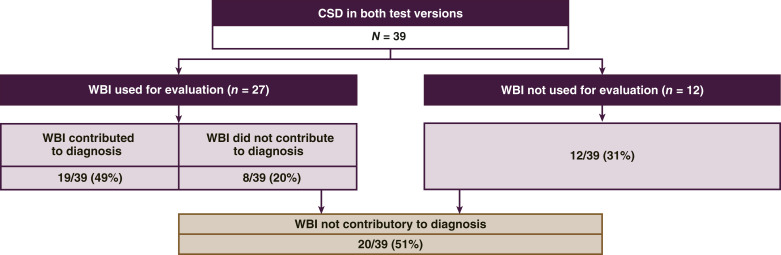
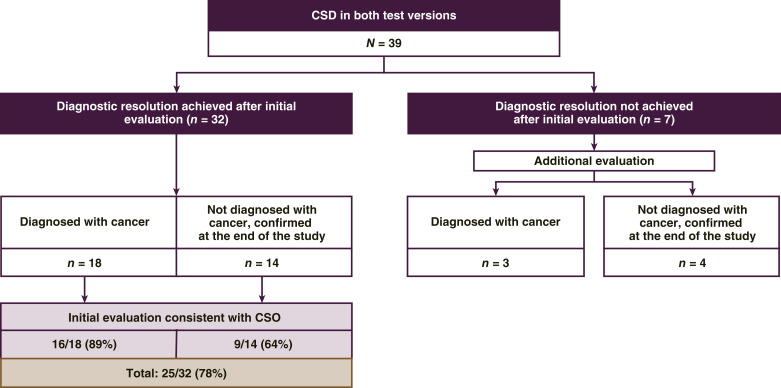
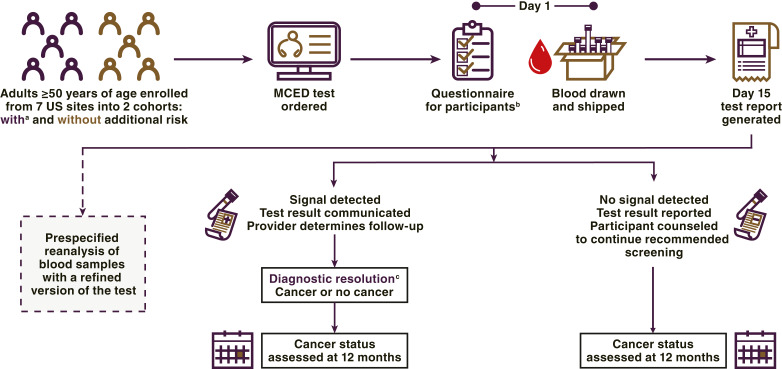
Blood-based multicancer early detection (MCED) tests represent a new approach for cancer detection. To gain insights into the utility of various approaches of evaluating a cancer signal detected (CSD) test result, we evaluated diagnostic journeys of a subset of 6,662 participants in PATHFINDER who had a CSD on both an initial and refined version of an MCED test that also provided a prediction of cancer signal origin (CSO). We sought to determine whether CSO prediction-guided diagnostic evaluations led to diagnostic resolution; whether participants with known risk factors for cancer beyond age alone and a negative initial diagnostic evaluation had a cancer diagnosis during study follow-up; the utility of whole-body imaging in reaching diagnostic resolution; and differences in the diagnostic journeys needed to reach diagnostic resolution for both true- and false-positive results. Of the 39 participants in this analysis, 82% (32/39) achieved diagnostic resolution after the initial evaluation, including 78% (25/32) who reached resolution specifically with a CSO prediction-directed workup. Eighteen percent (7/39) required additional evaluation for persistent clinical suspicion of cancer, all of whom achieved resolution (3 with and 4 without cancer). Whole-body imaging contributed to diagnostic resolution in only 49% of CSD cases. Approximately 90% of true- and false-positive cases had imaging tests; more true positives versus false positives (81.0% vs. 38.9%) had nonsurgical and/or surgical procedures. In conclusion, CSO prediction-directed evaluations enabled diagnostic resolution for most participants, although some with negative initial evaluations but persistent suspicion of cancer required additional testing.
Prevention relevance: MCED testing has the potential to increase detection of cancer at earlier stages. As MCED testing is a new technology, there are few data on the diagnostic journeys patients undergo following testing. We observed that for most patients, CSO prediction-directed workups were efficient, leading to diagnostic resolution after initial evaluation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


