{"title":"氟脱氧葡萄糖正电子发射断层扫描在胸腺上皮肿瘤治疗策略中的实用价值:在常规临床实践中更具体使用的意义","authors":"Kazuo Nakagawa","doi":"10.21037/med-24-46","DOIUrl":null,"url":null,"abstract":"<p><p>Many studies have demonstrated that 18-fluorine fluorodeoxyglucose positron emission tomography (FDG-PET) is useful for predicting the grade of malignancy of thymic epithelial tumors (TETs), and there is a close relationship between the maximum standardized uptake value (SUVmax) and tumor stage. However, more specific usage of FDG-PET for TETs has not been proposed, and the actual value of FDG-PET in routine clinical practice should be firmly clarified. In this review, following three cutoff values of SUVmax that may be helpful in determining treatment strategies in cases of anterior mediastinal masses, particularly presented as discrete and resectable lesions, are identified: (I) SUVmax of 7.5 as an indicator for pretreatment biopsy: differential diagnosis between TETs and mediastinal lymphoma (ML); (II) SUVmax of 4.2 as an indicator for a minimally invasive approach (MIA): differentiation of noninvasive TETs and invasive TETs; and (III) SUVmax of 5.9 as a reference value for the necessity of lymph node dissection (LND). There are still several challenges in using FDG-PET for routine clinical practice that need to be addressed, such as variations between instruments and institutions, leading to lower reproducibility. Harmonization methods should be applied to make clinical practice more uniform. Due to the rarity of these diseases, multi-institutional studies are warranted.</p>","PeriodicalId":74139,"journal":{"name":"Mediastinum (Hong Kong, China)","volume":"9 ","pages":"7"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11982993/pdf/","citationCount":"0","resultStr":"{\"title\":\"Practical value of fluorodeoxyglucose positron emission tomography in treatment strategies for thymic epithelial tumors: implications for more specific use in routine clinical practice.\",\"authors\":\"Kazuo Nakagawa\",\"doi\":\"10.21037/med-24-46\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Many studies have demonstrated that 18-fluorine fluorodeoxyglucose positron emission tomography (FDG-PET) is useful for predicting the grade of malignancy of thymic epithelial tumors (TETs), and there is a close relationship between the maximum standardized uptake value (SUVmax) and tumor stage. However, more specific usage of FDG-PET for TETs has not been proposed, and the actual value of FDG-PET in routine clinical practice should be firmly clarified. In this review, following three cutoff values of SUVmax that may be helpful in determining treatment strategies in cases of anterior mediastinal masses, particularly presented as discrete and resectable lesions, are identified: (I) SUVmax of 7.5 as an indicator for pretreatment biopsy: differential diagnosis between TETs and mediastinal lymphoma (ML); (II) SUVmax of 4.2 as an indicator for a minimally invasive approach (MIA): differentiation of noninvasive TETs and invasive TETs; and (III) SUVmax of 5.9 as a reference value for the necessity of lymph node dissection (LND). There are still several challenges in using FDG-PET for routine clinical practice that need to be addressed, such as variations between instruments and institutions, leading to lower reproducibility. Harmonization methods should be applied to make clinical practice more uniform. Due to the rarity of these diseases, multi-institutional studies are warranted.</p>\",\"PeriodicalId\":74139,\"journal\":{\"name\":\"Mediastinum (Hong Kong, China)\",\"volume\":\"9 \",\"pages\":\"7\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-03-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11982993/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Mediastinum (Hong Kong, China)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/med-24-46\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediastinum (Hong Kong, China)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/med-24-46","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Practical value of fluorodeoxyglucose positron emission tomography in treatment strategies for thymic epithelial tumors: implications for more specific use in routine clinical practice.
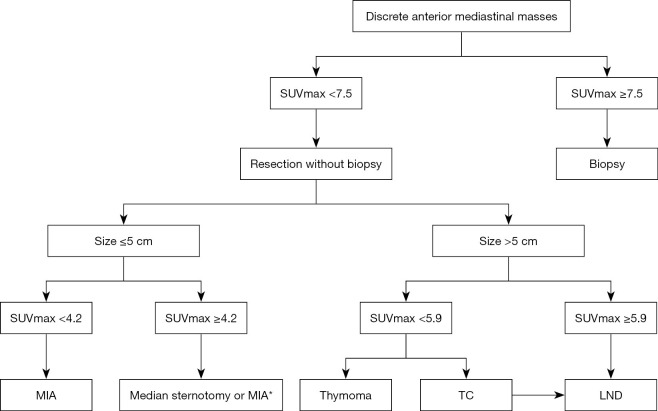
Many studies have demonstrated that 18-fluorine fluorodeoxyglucose positron emission tomography (FDG-PET) is useful for predicting the grade of malignancy of thymic epithelial tumors (TETs), and there is a close relationship between the maximum standardized uptake value (SUVmax) and tumor stage. However, more specific usage of FDG-PET for TETs has not been proposed, and the actual value of FDG-PET in routine clinical practice should be firmly clarified. In this review, following three cutoff values of SUVmax that may be helpful in determining treatment strategies in cases of anterior mediastinal masses, particularly presented as discrete and resectable lesions, are identified: (I) SUVmax of 7.5 as an indicator for pretreatment biopsy: differential diagnosis between TETs and mediastinal lymphoma (ML); (II) SUVmax of 4.2 as an indicator for a minimally invasive approach (MIA): differentiation of noninvasive TETs and invasive TETs; and (III) SUVmax of 5.9 as a reference value for the necessity of lymph node dissection (LND). There are still several challenges in using FDG-PET for routine clinical practice that need to be addressed, such as variations between instruments and institutions, leading to lower reproducibility. Harmonization methods should be applied to make clinical practice more uniform. Due to the rarity of these diseases, multi-institutional studies are warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


