Michael Hermsen, Patrick G Lyons, Govind Persad, Alice F Bewley, Chengsheng Mao, Kaveri Chhikara, Anoop Mayampurath, Matthew Churpek, Monica E Peek, Yuan Luo, William F Parker
{"title":"年龄与危重标准护理中的生命挽救:分诊评分预后准确性的多中心队列研究。","authors":"Michael Hermsen, Patrick G Lyons, Govind Persad, Alice F Bewley, Chengsheng Mao, Kaveri Chhikara, Anoop Mayampurath, Matthew Churpek, Monica E Peek, Yuan Luo, William F Parker","doi":"10.1097/CCE.0000000000001256","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Current protocols to triage life support use scores that are biased and inaccurate.</p><p><strong>Objectives: </strong>To determine if adding age to triage protocols used in disaster scenarios improves the identification of critically ill patients likely to survive.</p><p><strong>Design, setting, and participants: </strong>Observational cohort study from March 1, 2020, to March 1, 2022, at 22 hospitals in three networks, divided into derivation (12 hospitals) and validation cohorts (ten hospitals). Participants were critically ill adults (90% COVID-19 positive) who would have needed life support during an overwhelming case surge. Life support was defined as vasoactive medications for shock, invasive or noninvasive mechanical ventilation, or oxygen therapy with Pao2/Fio2 less than 200.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was death in the intensive care unit. We fit logistic regression models using a modified Sequential Organ Failure Assessment (SOFA) score with and without age in the derivation cohort and assessed predictive performance in the validation cohort using area under the receiver operating characteristic curves (AUCs) and compared observed and predicted mortality.</p><p><strong>Results: </strong>The final analysis contained 7,660 patients with 16,711 life-support episodes. In the validation cohort, the AUC for age plus SOFA was significantly higher than the AUC for SOFA alone (0.66 vs. 0.54; p < 0.001). SOFA score substantially overpredicted mortality (13% predicted vs. 5% observed) for younger patients (< 40 yr) and underestimated mortality (14% predicted vs. 31% observed) for older patients (> 80 yr). In contrast, age plus SOFA had good calibration overall and across age groups. The addition of age improved but did not eliminate differences between observed and predicted mortality across racial-ethnic groups.</p><p><strong>Conclusions and relevance: </strong>Age-inclusive triage better identifies ICU survivors than SOFA alone and is more equitable. Incorporating age into prioritization algorithms could save more lives in a crisis scenario.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 5","pages":"e1256"},"PeriodicalIF":2.7000,"publicationDate":"2025-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12074069/pdf/","citationCount":"0","resultStr":"{\"title\":\"Age and Saving Lives in Crisis Standards of Care: A Multicenter Cohort Study of Triage Score Prognostic Accuracy.\",\"authors\":\"Michael Hermsen, Patrick G Lyons, Govind Persad, Alice F Bewley, Chengsheng Mao, Kaveri Chhikara, Anoop Mayampurath, Matthew Churpek, Monica E Peek, Yuan Luo, William F Parker\",\"doi\":\"10.1097/CCE.0000000000001256\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Current protocols to triage life support use scores that are biased and inaccurate.</p><p><strong>Objectives: </strong>To determine if adding age to triage protocols used in disaster scenarios improves the identification of critically ill patients likely to survive.</p><p><strong>Design, setting, and participants: </strong>Observational cohort study from March 1, 2020, to March 1, 2022, at 22 hospitals in three networks, divided into derivation (12 hospitals) and validation cohorts (ten hospitals). Participants were critically ill adults (90% COVID-19 positive) who would have needed life support during an overwhelming case surge. Life support was defined as vasoactive medications for shock, invasive or noninvasive mechanical ventilation, or oxygen therapy with Pao2/Fio2 less than 200.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was death in the intensive care unit. We fit logistic regression models using a modified Sequential Organ Failure Assessment (SOFA) score with and without age in the derivation cohort and assessed predictive performance in the validation cohort using area under the receiver operating characteristic curves (AUCs) and compared observed and predicted mortality.</p><p><strong>Results: </strong>The final analysis contained 7,660 patients with 16,711 life-support episodes. In the validation cohort, the AUC for age plus SOFA was significantly higher than the AUC for SOFA alone (0.66 vs. 0.54; p < 0.001). SOFA score substantially overpredicted mortality (13% predicted vs. 5% observed) for younger patients (< 40 yr) and underestimated mortality (14% predicted vs. 31% observed) for older patients (> 80 yr). In contrast, age plus SOFA had good calibration overall and across age groups. The addition of age improved but did not eliminate differences between observed and predicted mortality across racial-ethnic groups.</p><p><strong>Conclusions and relevance: </strong>Age-inclusive triage better identifies ICU survivors than SOFA alone and is more equitable. Incorporating age into prioritization algorithms could save more lives in a crisis scenario.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 5\",\"pages\":\"e1256\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-05-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12074069/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001256\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001256","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
重要性:目前的生命支持使用分诊方案存在偏差和不准确。目的:确定在灾难场景中使用的分诊方案中增加年龄是否能提高对可能存活的危重患者的识别。设计、环境和参与者:观察性队列研究,从2020年3月1日至2022年3月1日,在三个网络中的22家医院进行,分为衍生队列(12家医院)和验证队列(10家医院)。参与者是危重的成年人(90%的COVID-19阳性),他们在病例激增期间需要生命支持。生命支持被定义为休克、有创或无创机械通气或Pao2/Fio2低于200的氧疗时血管活性药物。主要结局和指标:主要结局为重症监护病房死亡。我们在衍生队列中使用改进的有年龄和无年龄的顺序器官衰竭评估(SOFA)评分来拟合逻辑回归模型,在验证队列中使用受试者工作特征曲线(auc)下的面积来评估预测性能,并比较观察到的死亡率和预测的死亡率。结果:最终分析包含7660例患者,16711次生命支持发作。在验证队列中,年龄加SOFA的AUC显著高于单独SOFA的AUC (0.66 vs 0.54;P < 0.001)。SOFA评分明显高估了年轻患者(< 40岁)的死亡率(预测13%,观察到5%),低估了老年患者(80岁以下)的死亡率(预测14%,观察到31%)。相比之下,年龄加SOFA总体上和跨年龄组具有良好的校准。年龄的增加改善了但并没有消除种族-民族群体中观察到的和预测的死亡率之间的差异。结论和相关性:年龄分类比单独的SOFA更好地识别ICU幸存者,并且更公平。将年龄纳入优先排序算法可以在危机情况下挽救更多生命。
Age and Saving Lives in Crisis Standards of Care: A Multicenter Cohort Study of Triage Score Prognostic Accuracy.
Importance: Current protocols to triage life support use scores that are biased and inaccurate.
Objectives: To determine if adding age to triage protocols used in disaster scenarios improves the identification of critically ill patients likely to survive.
Design, setting, and participants: Observational cohort study from March 1, 2020, to March 1, 2022, at 22 hospitals in three networks, divided into derivation (12 hospitals) and validation cohorts (ten hospitals). Participants were critically ill adults (90% COVID-19 positive) who would have needed life support during an overwhelming case surge. Life support was defined as vasoactive medications for shock, invasive or noninvasive mechanical ventilation, or oxygen therapy with Pao2/Fio2 less than 200.
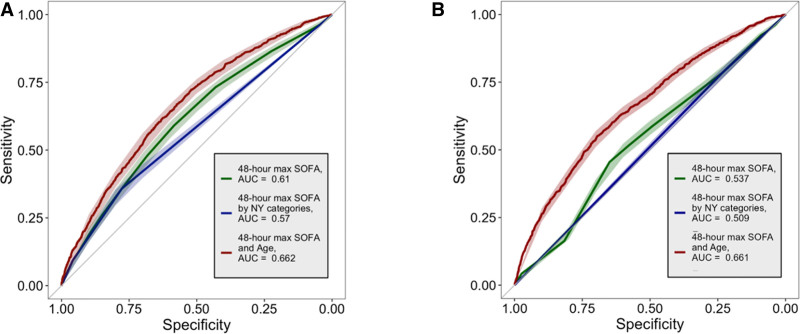
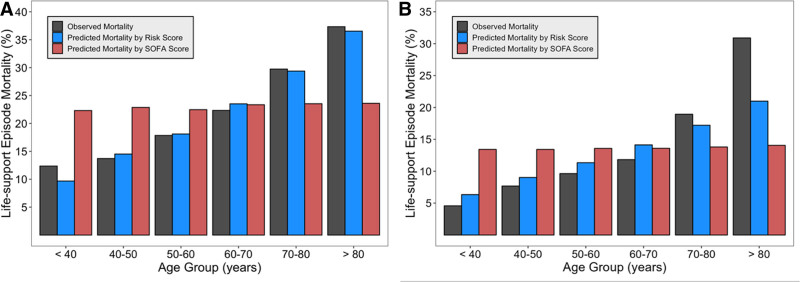
Main outcomes and measures: The primary outcome was death in the intensive care unit. We fit logistic regression models using a modified Sequential Organ Failure Assessment (SOFA) score with and without age in the derivation cohort and assessed predictive performance in the validation cohort using area under the receiver operating characteristic curves (AUCs) and compared observed and predicted mortality.
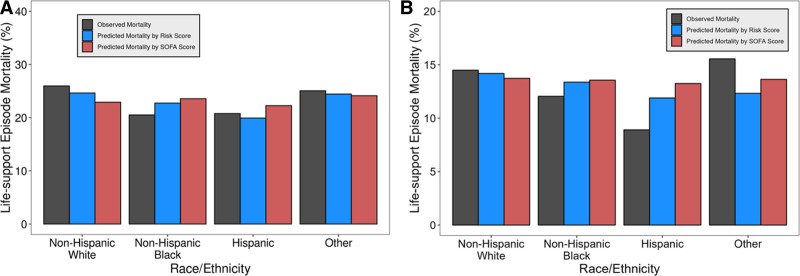
Results: The final analysis contained 7,660 patients with 16,711 life-support episodes. In the validation cohort, the AUC for age plus SOFA was significantly higher than the AUC for SOFA alone (0.66 vs. 0.54; p < 0.001). SOFA score substantially overpredicted mortality (13% predicted vs. 5% observed) for younger patients (< 40 yr) and underestimated mortality (14% predicted vs. 31% observed) for older patients (> 80 yr). In contrast, age plus SOFA had good calibration overall and across age groups. The addition of age improved but did not eliminate differences between observed and predicted mortality across racial-ethnic groups.
Conclusions and relevance: Age-inclusive triage better identifies ICU survivors than SOFA alone and is more equitable. Incorporating age into prioritization algorithms could save more lives in a crisis scenario.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


