{"title":"体感诱发电位是否与经颅运动诱发电位同时下降?日本脊柱外科及相关研究学会监测委员会的一项多中心研究","authors":"Hideki Shigematsu, Go Yoshida, Hiroki Ushirozako, Kenta Kurosu, Nobuaki Tadokoro, Masahiro Funaba, Shigenori Kawabata, Jun Hashimoto, Muneharu Ando, Shinichirou Taniguchi, Masahito Takahashi, Naoki Segi, Hiroaki Nakashima, Shiro Imagama, Shinji Morito, Kei Yamada, Tsunenori Takatani, Tsukasa Kanchiku, Yasushi Fujiwara, Hiroshi Iwasaki, Kanichiro Wada, Naoya Yamamoto, Kazuyoshi Kobayashi, Akimasa Yasuda, Kazuyoshi Nakanishi, Yasuhito Tanaka, Yukihiro Matsuyama, Katsushi Takeshita","doi":"10.22603/ssrr.2024-0229","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Multimodal intraoperative neurophysiological monitoring (IONM)-such as monitoring muscle-evoked potentials after transcranial electrical stimulation (Tc-MEP) with somatosensory-evoked potential (SEP) after electrical stimulation of the peripheral nerve-is recommended in spine surgeries to prevent iatrogenic neurological complications. However, the effect of using Tc-MEP with SEP to protect against neurological complications, particularly motor function, remains unknown. In clinical settings, changes due to Tc-MEP meeting the alarm points must be a potential neurological injury. This retrospective study, focusing on true-positive (TP) cases, aimed to clarify the change in the SEP waveform simultaneously with the Tc-MEP alarm.</p><p><strong>Methods: </strong>We included 68 patients with TP who had Tc-MEP changes and new postoperative motor weakness at more than one level of the manual muscle test after surgery. We compared the cases based on the category of spine surgery and paralysis type. We evaluated sex, age at spine surgery (high- or non high-risk), and paralysis type (segmental, long tract, or both). We defined the alarm points as follows: >70% decrease in Tc-MEP wave amplitudes, >50% decrease in wave amplitudes, or 10% extension of SEP latency. Next, we evaluated the SEP wave changes with a Tc-MEP alarm.</p><p><strong>Results: </strong>All patients showed progressive motor weakness after surgery, and 21 patients (31%) showed SEP changes at the same time as the Tc-MEP alarm. There were no statistically significant differences in the ratio of SEP change between the two groups according to the spine surgery category or among the three groups according to the paralysis type.</p><p><strong>Conclusions: </strong>Multimodal IONM is an important tool. However, the SEP changes do not necessarily appear immediately after the Tc-MEP alarm. Spine surgeons should appropriately treat Tc-MEP alarms to preserve motor function, regardless of SEP changes.</p>","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"9 2","pages":"173-178"},"PeriodicalIF":1.2000,"publicationDate":"2024-11-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11983110/pdf/","citationCount":"0","resultStr":"{\"title\":\"Does Somatosensory-Evoked Potential Simultaneously Decrease with Transcranial Motor-Evoked Potential Alarm? A Multicenter Study by the Monitoring Committee of the Japanese Society for Spine Surgery and Related Research.\",\"authors\":\"Hideki Shigematsu, Go Yoshida, Hiroki Ushirozako, Kenta Kurosu, Nobuaki Tadokoro, Masahiro Funaba, Shigenori Kawabata, Jun Hashimoto, Muneharu Ando, Shinichirou Taniguchi, Masahito Takahashi, Naoki Segi, Hiroaki Nakashima, Shiro Imagama, Shinji Morito, Kei Yamada, Tsunenori Takatani, Tsukasa Kanchiku, Yasushi Fujiwara, Hiroshi Iwasaki, Kanichiro Wada, Naoya Yamamoto, Kazuyoshi Kobayashi, Akimasa Yasuda, Kazuyoshi Nakanishi, Yasuhito Tanaka, Yukihiro Matsuyama, Katsushi Takeshita\",\"doi\":\"10.22603/ssrr.2024-0229\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Multimodal intraoperative neurophysiological monitoring (IONM)-such as monitoring muscle-evoked potentials after transcranial electrical stimulation (Tc-MEP) with somatosensory-evoked potential (SEP) after electrical stimulation of the peripheral nerve-is recommended in spine surgeries to prevent iatrogenic neurological complications. However, the effect of using Tc-MEP with SEP to protect against neurological complications, particularly motor function, remains unknown. In clinical settings, changes due to Tc-MEP meeting the alarm points must be a potential neurological injury. This retrospective study, focusing on true-positive (TP) cases, aimed to clarify the change in the SEP waveform simultaneously with the Tc-MEP alarm.</p><p><strong>Methods: </strong>We included 68 patients with TP who had Tc-MEP changes and new postoperative motor weakness at more than one level of the manual muscle test after surgery. We compared the cases based on the category of spine surgery and paralysis type. We evaluated sex, age at spine surgery (high- or non high-risk), and paralysis type (segmental, long tract, or both). We defined the alarm points as follows: >70% decrease in Tc-MEP wave amplitudes, >50% decrease in wave amplitudes, or 10% extension of SEP latency. Next, we evaluated the SEP wave changes with a Tc-MEP alarm.</p><p><strong>Results: </strong>All patients showed progressive motor weakness after surgery, and 21 patients (31%) showed SEP changes at the same time as the Tc-MEP alarm. There were no statistically significant differences in the ratio of SEP change between the two groups according to the spine surgery category or among the three groups according to the paralysis type.</p><p><strong>Conclusions: </strong>Multimodal IONM is an important tool. However, the SEP changes do not necessarily appear immediately after the Tc-MEP alarm. Spine surgeons should appropriately treat Tc-MEP alarms to preserve motor function, regardless of SEP changes.</p>\",\"PeriodicalId\":22253,\"journal\":{\"name\":\"Spine Surgery and Related Research\",\"volume\":\"9 2\",\"pages\":\"173-178\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-11-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11983110/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine Surgery and Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22603/ssrr.2024-0229\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/27 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2024-0229","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/27 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Does Somatosensory-Evoked Potential Simultaneously Decrease with Transcranial Motor-Evoked Potential Alarm? A Multicenter Study by the Monitoring Committee of the Japanese Society for Spine Surgery and Related Research.
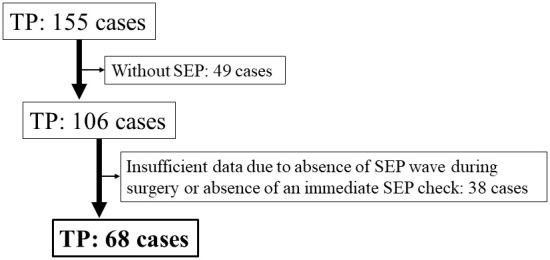
Introduction: Multimodal intraoperative neurophysiological monitoring (IONM)-such as monitoring muscle-evoked potentials after transcranial electrical stimulation (Tc-MEP) with somatosensory-evoked potential (SEP) after electrical stimulation of the peripheral nerve-is recommended in spine surgeries to prevent iatrogenic neurological complications. However, the effect of using Tc-MEP with SEP to protect against neurological complications, particularly motor function, remains unknown. In clinical settings, changes due to Tc-MEP meeting the alarm points must be a potential neurological injury. This retrospective study, focusing on true-positive (TP) cases, aimed to clarify the change in the SEP waveform simultaneously with the Tc-MEP alarm.
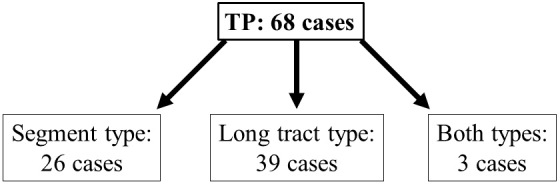
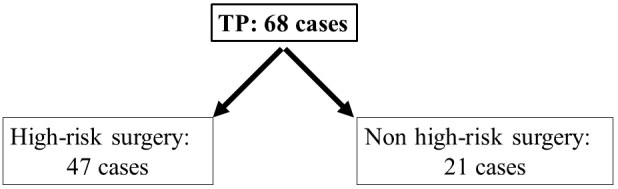
Methods: We included 68 patients with TP who had Tc-MEP changes and new postoperative motor weakness at more than one level of the manual muscle test after surgery. We compared the cases based on the category of spine surgery and paralysis type. We evaluated sex, age at spine surgery (high- or non high-risk), and paralysis type (segmental, long tract, or both). We defined the alarm points as follows: >70% decrease in Tc-MEP wave amplitudes, >50% decrease in wave amplitudes, or 10% extension of SEP latency. Next, we evaluated the SEP wave changes with a Tc-MEP alarm.
Results: All patients showed progressive motor weakness after surgery, and 21 patients (31%) showed SEP changes at the same time as the Tc-MEP alarm. There were no statistically significant differences in the ratio of SEP change between the two groups according to the spine surgery category or among the three groups according to the paralysis type.
Conclusions: Multimodal IONM is an important tool. However, the SEP changes do not necessarily appear immediately after the Tc-MEP alarm. Spine surgeons should appropriately treat Tc-MEP alarms to preserve motor function, regardless of SEP changes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


