Jillian McNally, David Wilson, Emma E Jones, Neyousha Shahisavandi, Caroline King, Chad Coles, Raymond Andrew Glennie
{"title":"基于视频的骨科手术技能评估:捕捉关键手术细节的技术指南。","authors":"Jillian McNally, David Wilson, Emma E Jones, Neyousha Shahisavandi, Caroline King, Chad Coles, Raymond Andrew Glennie","doi":"10.2106/JBJS.OA.24.00183","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Surgical skills are critical to assess in residency programs. These observations often occur in the clinical settings, which are limited by patient safety and potential bias. High fidelity simulated cadaveric surgery can account for some of these shortcomings. Professional video offers a promising avenue to both anonymize and effectively evaluate surgical skill. The objective of this study were to describe the technique for professional video capture of simulated, open orthopaedic surgeries and to assess construct validity by comparing objective performance scores from the videos with the learner's stage of training.</p><p><strong>Methods: </strong>In 2022, one experienced surgeon and 3 trainees (post graduate year [PGY]-4, PGY-3, PGY-2) were recruited from a residency program to perform 2 moderately challenging surgeries (open reduction and internal fixation of both bone forearm and talus fractures), with fractures simulated using an osteotome. Videographers positioned cameras at various positions throughout a skills laboratory. Total costs were calculated. Statistical analysis was performed to compare evaluator scores of participants' actual level of training.</p><p><strong>Results: </strong>The simulated surgeries were recorded, edited for optimal viewing angles, and anonymized by blurring faces and voice over technology. Seventeen local teaching faculty were recruited to evaluate the videos. The videos were shortened on average 65 minutes for critical steps to be represented in the final production (i.e., Bone reduction, dissection of neurovascular structures, radiographic images, etc.) The full cost to produce the 8 surgical videos was $48,934.00 Canadian dollars. The final data set had 61 observations, with a range of 13 to 17 observations per participant. There was a 19.7% error rate, meaning the videos were generally 80% accurate in predicting the year of training.</p><p><strong>Conclusions: </strong>The discriminative ability of the videos was better at detecting true \"novice\" and \"expert\" surgeons but less accurate between the middle years of training. A larger, multicentered study with more participants is needed to draw any further conclusions.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 2","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020707/pdf/","citationCount":"0","resultStr":"{\"title\":\"Video-Based Assessment of Surgical Skill in Orthopaedic Surgery: A Technique Guide to Capturing Critical Surgical Detail.\",\"authors\":\"Jillian McNally, David Wilson, Emma E Jones, Neyousha Shahisavandi, Caroline King, Chad Coles, Raymond Andrew Glennie\",\"doi\":\"10.2106/JBJS.OA.24.00183\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Surgical skills are critical to assess in residency programs. These observations often occur in the clinical settings, which are limited by patient safety and potential bias. High fidelity simulated cadaveric surgery can account for some of these shortcomings. Professional video offers a promising avenue to both anonymize and effectively evaluate surgical skill. The objective of this study were to describe the technique for professional video capture of simulated, open orthopaedic surgeries and to assess construct validity by comparing objective performance scores from the videos with the learner's stage of training.</p><p><strong>Methods: </strong>In 2022, one experienced surgeon and 3 trainees (post graduate year [PGY]-4, PGY-3, PGY-2) were recruited from a residency program to perform 2 moderately challenging surgeries (open reduction and internal fixation of both bone forearm and talus fractures), with fractures simulated using an osteotome. Videographers positioned cameras at various positions throughout a skills laboratory. Total costs were calculated. Statistical analysis was performed to compare evaluator scores of participants' actual level of training.</p><p><strong>Results: </strong>The simulated surgeries were recorded, edited for optimal viewing angles, and anonymized by blurring faces and voice over technology. Seventeen local teaching faculty were recruited to evaluate the videos. The videos were shortened on average 65 minutes for critical steps to be represented in the final production (i.e., Bone reduction, dissection of neurovascular structures, radiographic images, etc.) The full cost to produce the 8 surgical videos was $48,934.00 Canadian dollars. The final data set had 61 observations, with a range of 13 to 17 observations per participant. There was a 19.7% error rate, meaning the videos were generally 80% accurate in predicting the year of training.</p><p><strong>Conclusions: </strong>The discriminative ability of the videos was better at detecting true \\\"novice\\\" and \\\"expert\\\" surgeons but less accurate between the middle years of training. A larger, multicentered study with more participants is needed to draw any further conclusions.</p>\",\"PeriodicalId\":36492,\"journal\":{\"name\":\"JBJS Open Access\",\"volume\":\"10 2\",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020707/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBJS Open Access\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2106/JBJS.OA.24.00183\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.24.00183","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Video-Based Assessment of Surgical Skill in Orthopaedic Surgery: A Technique Guide to Capturing Critical Surgical Detail.
Introduction: Surgical skills are critical to assess in residency programs. These observations often occur in the clinical settings, which are limited by patient safety and potential bias. High fidelity simulated cadaveric surgery can account for some of these shortcomings. Professional video offers a promising avenue to both anonymize and effectively evaluate surgical skill. The objective of this study were to describe the technique for professional video capture of simulated, open orthopaedic surgeries and to assess construct validity by comparing objective performance scores from the videos with the learner's stage of training.
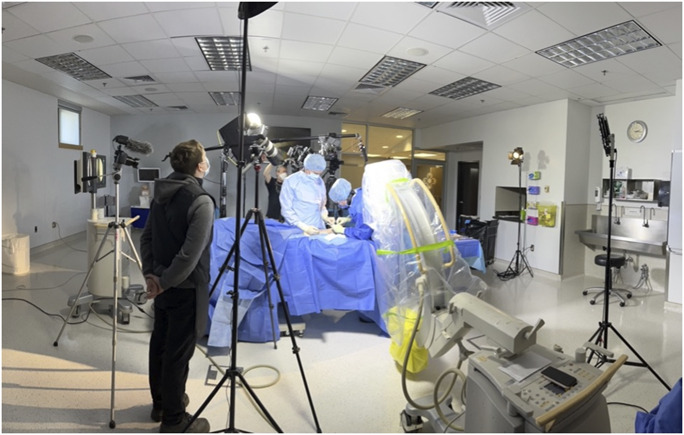
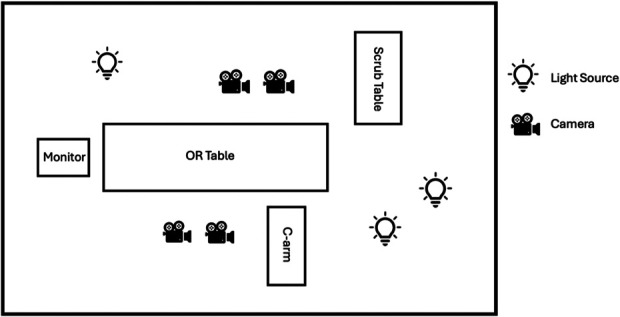
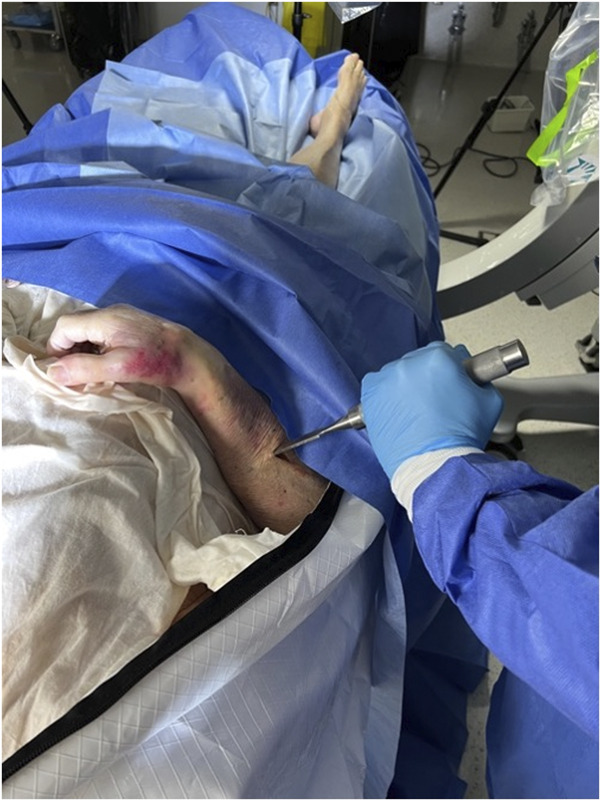
Methods: In 2022, one experienced surgeon and 3 trainees (post graduate year [PGY]-4, PGY-3, PGY-2) were recruited from a residency program to perform 2 moderately challenging surgeries (open reduction and internal fixation of both bone forearm and talus fractures), with fractures simulated using an osteotome. Videographers positioned cameras at various positions throughout a skills laboratory. Total costs were calculated. Statistical analysis was performed to compare evaluator scores of participants' actual level of training.
Results: The simulated surgeries were recorded, edited for optimal viewing angles, and anonymized by blurring faces and voice over technology. Seventeen local teaching faculty were recruited to evaluate the videos. The videos were shortened on average 65 minutes for critical steps to be represented in the final production (i.e., Bone reduction, dissection of neurovascular structures, radiographic images, etc.) The full cost to produce the 8 surgical videos was $48,934.00 Canadian dollars. The final data set had 61 observations, with a range of 13 to 17 observations per participant. There was a 19.7% error rate, meaning the videos were generally 80% accurate in predicting the year of training.
Conclusions: The discriminative ability of the videos was better at detecting true "novice" and "expert" surgeons but less accurate between the middle years of training. A larger, multicentered study with more participants is needed to draw any further conclusions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


